Anesthesia Deaths Audit at Niamey National Hospital
Author'(s): Daddy H1*, Chaïbou MS1, Gagara M1, Nainou Guero A1, Younsa H2, Kadi I2 and Sani R2
1Department of Anesthesia, Niamey National Hospital, Niger,Republic.
2Département of Surgery, Niamey National Hospital, Niger, Republic.
*Correspondence:
Dr. DADDY Hadjara, Anesthesia Department, Niamey National Hospital.
Received: 27 April 2020; Accepted: 15 May 2020
Citation: Daddy H, Chaïbou MS, Gagara M, et al. Anesthesia Deaths Audit at Niamey National Hospital. Anesth Pain Res. 2020; 4(1):1-4.
Abstract
Objective: The aim of this study is to audit the perioperative deaths of patients operated on at Niamey National Hospital (HNN).
Patients and Methods: This is a cross-sectional prospective study from January to December, 2018; one (1) year. Have been included all patients who died in operating room or within 24 hours of surgery. Audit team is composed of a senior surgeon and two anesthetists. The following variables were studied: age, sex, patient history, American Society of Anesthesiologists (ASA) classification, Mallampati score, surgical indication, type of anesthesia, induction and maintenance drugs, perioperative incidents and accidents, imputation and cause of death. Data were analyzed with Word 2007 and Epi Info 6TM (Centers for Disease Control and Prevention Atlanta, GA).
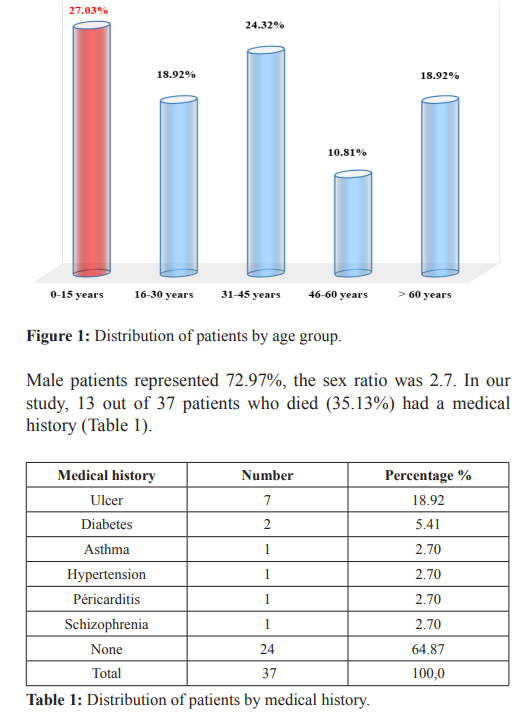
Results: During the period of our study, 5411 patients had been operated. There were 37 perioperative deaths, a frequency of 0.68%. The average age of death patients was 27.52 years, with a sex ratio of 2.7. Digestive surgery was the most concerned followed by neurosurgery with 67.57% and 13.51% respectively. Surgery was performed in emergency in 89.19% and elective in 10.81% of cases. Patients were classified ASA1 in 8.11%; ASA2 in 40.54% and ASA3 in 27.03%. All of death patients were operated on under general anesthesia. Hypotension was the most common incident in the intraoperative and postoperative periods, with 51.35% and 18.92% respectively. Nineteen patients (51.35%) died on the operating table; including 6 at induction, 18 patients died postoperatively (48.65%). Deaths were related to the evolution of the patient's pathology in 70.27% (n = 26), to surgery in 16.22% (n = 6) and anesthesia in 13.51% (n = 5).
Conclusion: Death audit reveals multiple and varied causes, the improvement of this situation requires training and equipping our hospitals with suitable materials and consumables.
Keywords
Introduction
Since the beginning of time, one of the major concerns of man has been to relieve pain or to remove it. But it took October 16th, 1846 to speak of the historical discovery of anesthesia, which is a discipline that takes these concerns into account. This young discipline thus born experienced many difficulties during its evolution, including among other things the control of perioperative risks and deaths.
Apart from all these difficulties, progress has been made in this area, nowadays allowing the anesthetic management of increasingly fragile patients with more severe lesions with a significant reduction in death. Despite the progress intraoperative deaths remain a frequent situation and present multivariate causes. Most often these deaths are wrongly attributed to anesthesia or surgery acts [1,2].
Patients and Methods
This is a cross-sectional prospective study from January to December, 2018, either one (1) year. Have been included patients who underwent general or locoregional anesthesia for scheduled or urgent surgery, who died either during anesthesia or within 24 hours of surgery. The data collected were analyzed by an expert committee (composed of a surgeon senior and two anesthetist’s senior). The following variables were studied: age, sex, patient history, American Society of Anesthesiologists (ASA) status, Mallampati score, surgical indication, type of anesthesia, induction and maintenance drugs, perioperative incidents and accidents, imputation and cause of death. Data were analyzed with Word 2007 and Epi Info 6™ (Centers for Disease Control and Prevention Atlanta, GA).
Results
In this study, 5411 patients were operated, including 37 perioperative deaths (0.68%). The most represented age group was that of 0 to 15 years old (Figure 1). The average age of patient deaths was 27.52 years with extremes of 1 year and 65 years.
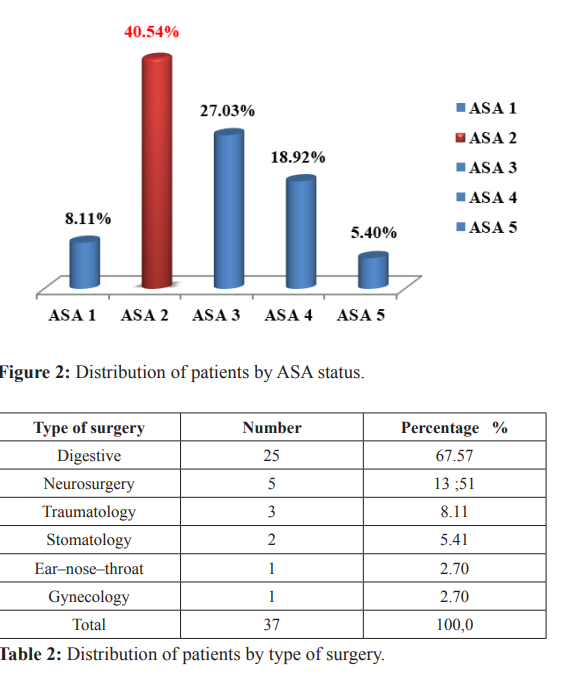
Patients classified Mallampati 1 represented 70.27% of cases (n = 26), Mallampati 2; 24.32% (n = 9) and Mallampati 3; 5.41% (n = 2). The patients were ASA1 in 8.11%; ASA 2 in 40.54% and ASA 3 in 27.03% (Figure 2).
Surgery was performed urgently in 89.19% and elective in 10.81% of cases. Digestive surgery was the most performed followed by neurosurgery with 67.57% and 13.51% respectively (Table 2).
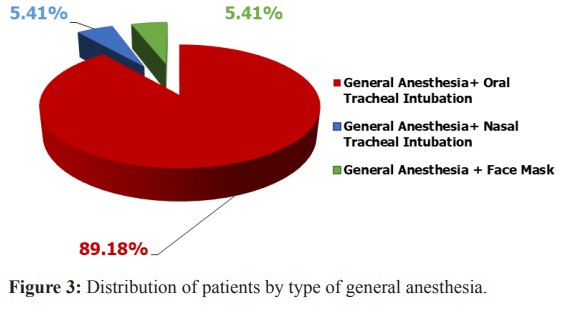
All of deaths were operated under general anesthesia. The most commonly used protocol was general anesthesia with orotracheal intubation (Figure 3). Anesthesia was performed by senior anesthetist nurses in 86.50% of cases and by anesthetists in 13.50%. Intravenous induction was performed with ketamine and propofol in 67.57% and 21.62% of patients, respectively.
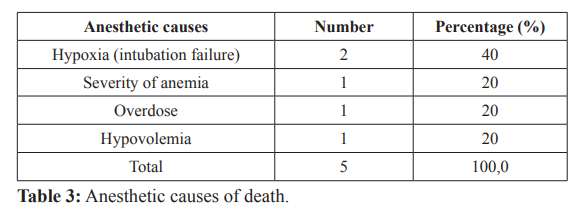
The maintenance was with volatile anesthetics in 84.78% of patients and ketamine in 5.41% associated with analgesics. The most widely used curare’s were induction suxamethonium with 83.78% of cases and atracurium in maintenance in 24.33% of patients. Hypotension was the most common incident in the intraoperative and postoperative periods, with 51.35% and 18.92% respectively. The average anesthesia duration was 92 min. Nineteen patients (51.35%) died during the anesthesia, six of which occurred during induction; 18 patients died postoperatively (48.65%). Deaths were related to the evolution of the patient's pathology in 70.27% (n = 26), to surgery in 16.22% (n = 6) and to anesthesia in 13.51% (n= 5). The anesthetic cause was post-operative hypoxia (2 out of 5 patients) (Table 3). The cause of death related to the surgery was mainly hemorrhaged in connection with a defect in hemostasis.
Discussion
In our study, death during anesthesia represented 0.68%. This result is lower than that found by the ASOS study in 2018 which found a rate of 1.1% for Niger republic. It is also lower than that of Ouro-Bang’na A. F. et al. who found a frequency of 0.89%. This result is superior to those reported by other authors [3-6]. The average age was 27.52 years with extremes of 1 year and 65 years. Male patients represented 72.97%. Hicham K. et al. also found this predominance of the male sex with 63.36%. On the other hand, the Togo series had found a predominance of the female sex with 58% of women [4,6]. This could be explained by the absence of an obstetrics department at the Niamey National Hospital. In our series, patients classified ASA 2 represented 43.2%. Hicham K. et al. also found this predominance of class ASA 2 (59%). Emergency surgery predominated with 89.20%. In Togo, too, a predominance of emergency surgery has been found. The risk of perioperative complications was higher for emergency procedures [4]. All of our deceased patients were operated on under general anesthesia, indeed a risk of complications and death has been shown compared to spinal anesthesia [7]. Anesthesia was performed by a nurse anesthetist in 86.50% of the cases and 13.50% by anesthetist. Bonkoungou P. et al. reported 71.6% of anesthesia performed by nurse anesthetists. This reflects the insufficient number of anesthetists in hospitals of most developing countries [8,9]. The analgesics used intraoperatively were mainly fentanyl and sufentanil with 45.94% and 43.24% respectively. This result is different from previous series in the same hospital, which mainly found fentanyl as the analgesic used [10,11]. Hypotension was the most common adverse event intraoperatively (51.35%). EhounoudH. et al. found this predominance of hypotension with 62.5% [12]. In the immediate post-operative period, hypotension was the most common adverse event in our study, with a rate of 18.92%. A study taking into account immediate post-operative adverse events also found this predominance of hypotension with a rate of 33.33% [5]. More than half of the deaths recorded (51.35%) had occurred on the operating table; 37.84% occurred within 6 hours post-operative; 8.11% occurred between 6 and 12 hours post- operatively and 2.70% occurred between 12- and 24-hours post- operative. This result is different from that of Ourobang’na A. F. et al. who found a predominance of deaths in the post-interventional surveillance room with 75% and 25% in the operating room [4].
The deaths were linked to the patient's pathology, 70.27% (n = 26) of the cases. Surgery was involved for six deaths (16.22%), anesthesia for five deaths (13.51%). The predominance of deaths related to the development of the patient's pathology could be explained by the delay in consultation and patient management.
The respiratory cause (hypoxia due to intubation failure) was the most common anesthetic cause in 40% of cases. The other causes of death due to anesthesia were: an error in assessing the severity of decompensated anemia (20%), an overdose (20%) and non- compliant management of hypovolemia (20%). Unlike our series, Gounajjar found a predominance of cardiovascular causes with 60% followed by respiratory causes with 27% [13]. The surgery- related death was due to hemorrhage related to either accidental injury to a vessel and lack of surgical hemostasis. Ouro-Bang’naA. F. et al. also found poorly controlled bleeding as the primary cause of surgery-related deaths [4].
Conclusion
The death audit reveals multiple and varied causes, improving this situation requires raising public awareness to consult early, but also by improving the technical platform, training in sufficient numbers of anesthetists, continuing education of all the actors of health but also the continuity of the audit of the deaths at the level of the operating theater.
References
1.Desai SP, Desai MS, Maddi R, et al. A tale of two paintings: depictions of the first public demonstration of ether anesthesia. Anesthesiology. 2007; 106: 1046-1050.
2.Morel J, Dupont G, Passot S, et al. l’Anesthésie influe t-elle la mortalité péri opératoire? Département d’Anesthésie et de Réanimation, CHU Hôpital Nord, Conférences d’actualisation 2015.
3.Biccard BM, Madiba TE, Kluyts HL, et al. Perioperative patient outcomes in the African Surgical Outcomes Study: a 7-day prospective observational cohort study. Lancet. 2018; 391: 1589-1598.
4.Ouro-Bang’na Maman AF, Agbe´tra N, Egbohou P, et al. Morbidité–mortalité péri opératoire dans un pays en développement : expérience du CHU de Lomé (Togo). Annales francaises d'anesthesie et de reanimation. 2008; 27: 1030-1033.
5.Diallo B, Keita M, Dicko H, et al. Classification de l’American Society of Anesthesiologists et évènements indésirables péri-opératoires en anesthésie programmée au Mali. [Classification of American Society of Anesthesiologists and Perioperative Adverse Events Scheduled In Anesthesia]. Rev Afr Anesthésiol Med Urgence. 2013; 39-45.
6.Kechna H, Ouzzad O, Chkoura K, et al. Evénements indésirables peropératoires: lecture critique du registre du bloc opératoire de l’hôpital militaire Moulay Ismail Meknès. [peroperative adverse events: critical reading of the operating room register at the Moulay Ismail Meknes military hospital]. The Pan African Medical Journal. 2016; 24: 178.
7.Otiobanda GF, Elombila M, Mpoy Emy Monkessa CM, et al. Complications observées en salle de surveillance post- Interventionnelle du Centre Hospitalier Universitaire de Brazzaville. [Complications occuring at post anesthesia care unit in University Hospital at Brazzaville]. Rev Afr Anesth Méd Urg. 2019.
8.Bonkoungou P, Lankondé M, Ki KB, et al. Prise en charge anesthésique des abdomens aigus chirurgicaux dans un hôpital de référence nationale au Burkina-Faso. [Anaesthesia management for acute surgical abdomen in a referra hospital in Burkina -Faso]. Rev Afr Anesth Méd Urg. 2017; 18-24.
9.Adnet P, Diallo A, Sanou J, et al. Pratique de l’anesthésie par les infirmiers(e)s en Afrique francophone subsaharienne. [Anaesthesia practice by nurse anaesthetists in French speaking sub-Saharan Africa]. Ann Fr Anesth Réanim. 1999; 18: 636–641.
10.Chaibou MS, Daddy H, James Didier L, et al. Anaesthetic management of homozygous sickle cell patients at Niamey National Hospital. African Journal of Anaesthesia and Intensive Care. 2016; 7-9.
11.Chaibou MS, Bako H, Daddy H, et al. Anesthésie du sujet âgé à l’Hôpital National de Niamey : A propos de 119 cas. [Anaesthesia in older patients at Niamey National Hospital: Prospective study about 119 cases]. Rev Afr Anesthésiol Med Urgence. 2017; 14-17.
12.Ehounoud H, Yapo YP, Itéké F, et al. Evaluation des complications péri-opératoires de la chirurgie d’exérèse pulmonaire à l’institut de cardiologie d’Abidjan. [Evaluation of complications of lung resection surgery at cardiologic institute of Abidjan]. Rev Afr Anesthésiol Med Urgence. 2013; 24-28.
13.Gounajjar. Mahfoud Mortalité liée à l'anesthésie Casablanca (A propos de 152 582 anesthésies), Thèse de doctorat en Médecine. Faculté de Médecine et de Pharmacie, Université Hassan II, Casablanca, 2005.