Aortic Dissection Involving a Right Retroesophagian Subclaviary Artery (LUSORIA) Associated with a Bi-Carotidian Trunk: About a Case at the National University Hospital Center of Fann (Sénégal)
Author'(s): Sarr El Hadj Mbacké1, Khaddra H1, Manga Simon Joël2*, Seye Modou1, Dioum Momar1, Ba MD1, Sy Sidy Lamine1, Bindia Dominique1, Sarr Ndeye Arame1, Tine Elisabeth Arame1, Diallo Arame Diagne1, Ba Kadia1, Dieye Ousmane1 and Diop Ibrahima Bara1
1Cardiologie departement, Fann national university center, Dakar Cheikh Anta Diop University, Dakar, Sénégal.
2Cardiology departement, Hospital de la Paix, Assane Seck University of Ziguinchor, Ziguinchor, Sénégal.
*Correspondence:
Dr Simon Joël MANGA, Cardiology departement, Hospital de la Paix, Assane Seck University of Ziguinchor, BP 523, Sénégal, Tel:+221 77 650 25 32.
Received: 15 October 2021; Accepted: 20 November 2021
Citation: : Mbacké SEH, Khaddra H, Joël MS, et al. Aortic Dissection Involving a Right Retroesophagian Subclaviary Artery (LUSORIA) Associated with a Bi-Carotidian Trunk: About a Case at the National University Hospital Center of Fann (Sénégal). Cardiol Vasc Res. 2021; 5(6): 1-5.
Abstract
The lusoria artery is a rare congenital vascular anomaly involving most of the time the right subclavian artery. It can also be associated with a serious vascular pathology such as aortic dissection although this phenomenon is not common in the literature and most often requires rather complex surgical management because of the layout of this artery. We report a discovery of a lusoria artery case revealed by aortic dissection. This is a 63-yearold patient with recently discovered hypertension as a cardiovascular risk factor. He was received for severe chest pain. Clinical examination found grade III systolo-diastolic hypertension and tachycardia. The thoracic CT angiography found an aspect of type B aortic dissection associated with an aberrant right subclavian artery of the lusoria type. In emergency, the patient had benefited from an antihypertensive treatment allowing stabilizing his high blood pressure.
The development during hospitalization was favorable with a disappearance of the pain and a stabilization of his blood pressure levels. His discharge was made on D10 of hospitalization with a transfer to a cardiovascular surgery center for better treatment.
Keywords
Introduction
The aortic arch and its branches can be the site of anatomical variations. The most common anomaly concerns the right subclavian artery, which originates directly from the aorta and thus joins the upper right limb by taking a retro-esophageal path. Its incidence is of the order of 0.5 to 2% in the general population and can be associated in 30% of cases with a bi-carotid trunk. It is most often asymptomatic and discovered by chance [1].
The most classic and well-known manifestation is dysphagia and the delay in its occurrence may be due to an elevation of the aortic arch associated with age, whether or not associated with arterial hypertension [2,3].
The lusoria artery may also be the site of an inherent although non- specific pathology of an atherosclerotic, traumatic or inflammatory nature [4,5]. She may also be interested in the extension of an aortic dissection and the most specific and serious lesion of the aberrant right subclavian artery in adults is the aneurysm [6,7].
Congenital vascular anomalies are not a cause favoring the dissection but can give it particular clinical and radiological aspects. The particular form of an extension to an aberrant right subclavian artery of the lusoria type is an exceptional possibility [8].
Thus, in the literature, only 16 described cases of a lusoria artery and aortic dissection have been found, and this poses a problem in the context of possible surgical management [7].
Observation
This is a 63-year-old patient with recently discovered high blood pressure on dual antihypertensive therapy (ACE inhibitor and calcium channel blocker) who presented, a month earlier, with stabbing chest pain, stabbing in the back and exacerbated by cough. The patient does not describe dysphagia and in view of this symptomatology, he consulted the SAU of the Pikine Hospital where a thoracic CT angiography was performed. In front of the results, he was referred to us for better support.
Clinical examination on arrival revealed grade 3 systolo-diastolic HBP and auscultatory tachycardia.
The electrocardiogram (ECG) on arrival showed regular sinus tachycardia with a heart rate of 120 cycles / min, QRS axis normal, PR fixed at 14/100 sec and an atrial and left ventricular hypertrophy (Figure 1).
Transthoracic ultrasound appeared in favor of thoracic and abdominal aortic dissection over hypertensive cardiomyopathy. The presence of an intimal flap separating a true channel (1/3) and a false channel (2/3) on a non-aneurysmal aorta (Figure 2).
The thoracoabdominal CT angiography showed a dissection of the thoracic and abdominal aorta type B of Stanford with an intimal flap extended from segment II (at the ostium foot otf the artery under left clavian) to segment V (in addition to the lower mesenteric) (Figure 3). The flap also involved the origin of the right subclavian, celiac artery, superior mesenteric artery and renal arteries. There was the presence of atherosclerotic infiltrate with locally calcified aortic plaques and absence of aneurysm, thrombosis or hemorrhage.
The analysis of the thoracic sections in the mediastinal window after injection of iodinated contrast product also revealed an anatomical variant of the arrangement of the supra-aortic trunks with an anterior trunk giving both common carotids (Figure 4) and two subclavian arteries with specific origins including a right lusoria artery (Figure 5).
Doppler ultrasound of the renal arteries found a 34.3 mm infra- renal abdominal aortic aneurysm with dissection (Figure 6).
In emergency, the patient was hospitalized in a cardiological intensive care unit (ICU), conditioned and aggressive blood pressure control was undertaken with the initiation of a central acting IV antihypertensive drug (Nicardipine) to PSE and a relay with a triple anti-hypertensive therapy made of IEC, I.C and beta- blocker with a systolic blood pressure (SBP) target figure of less than or equal to 120 mm Hg.
The exeat was scheduled after 10 days of hospitalization with stabilization of these blood pressure levels under antihypertensive quadruple therapy.
The patient left with a referral to a cardiovascular surgery center for more adequate management.

Figure 1: Electro cardio gramm.
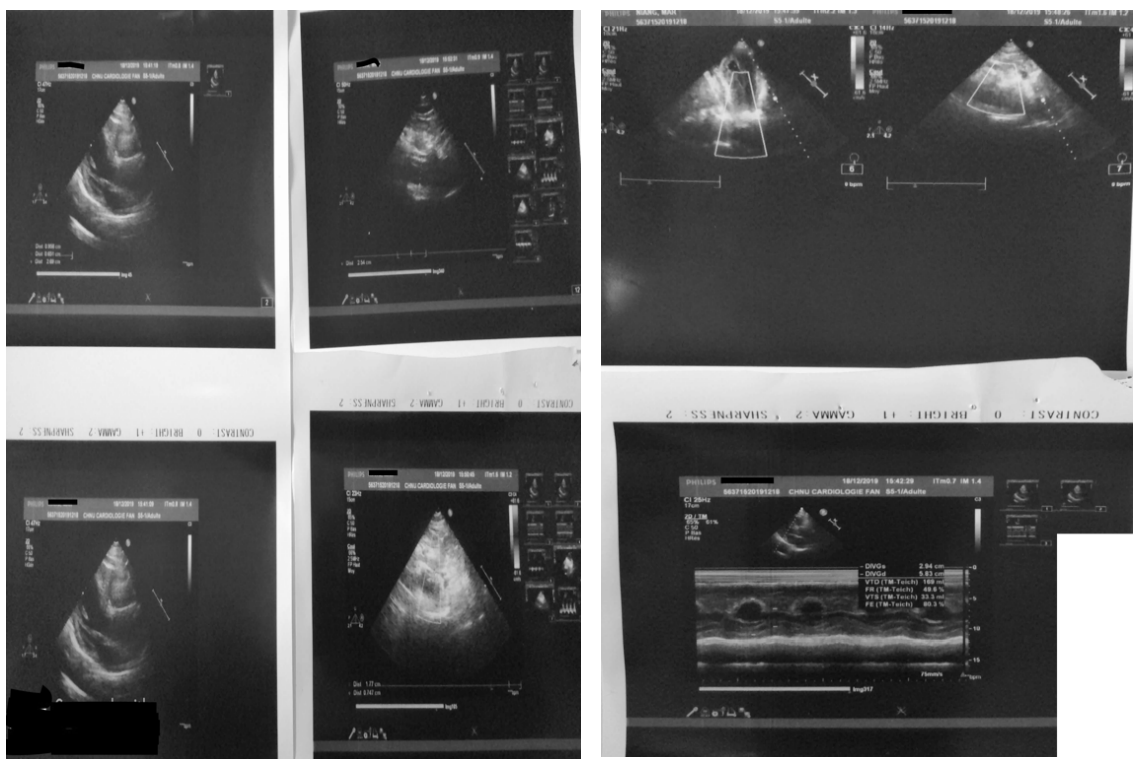
Figure 2: Transthoracic ultrasound.
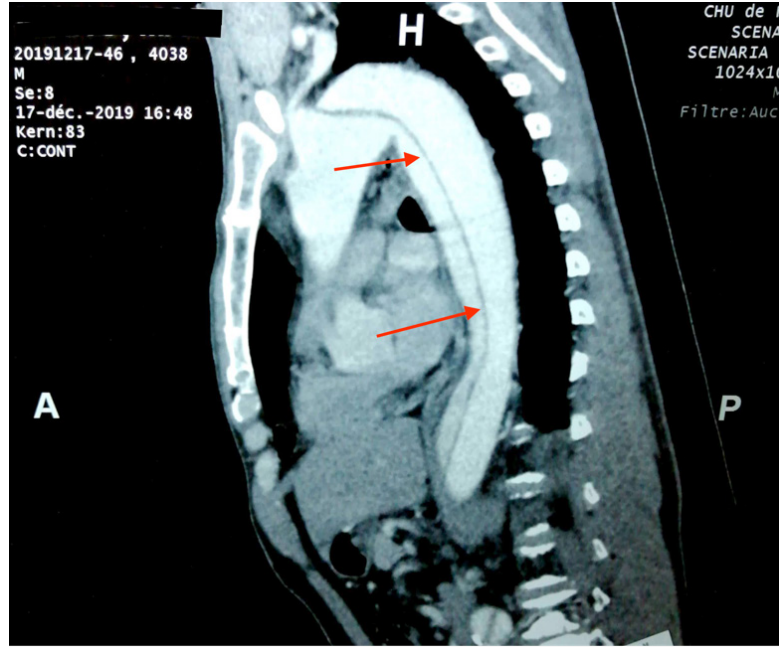
Figure 3: Thoracic angioscan (Thoracoabdominal aortic dissection).
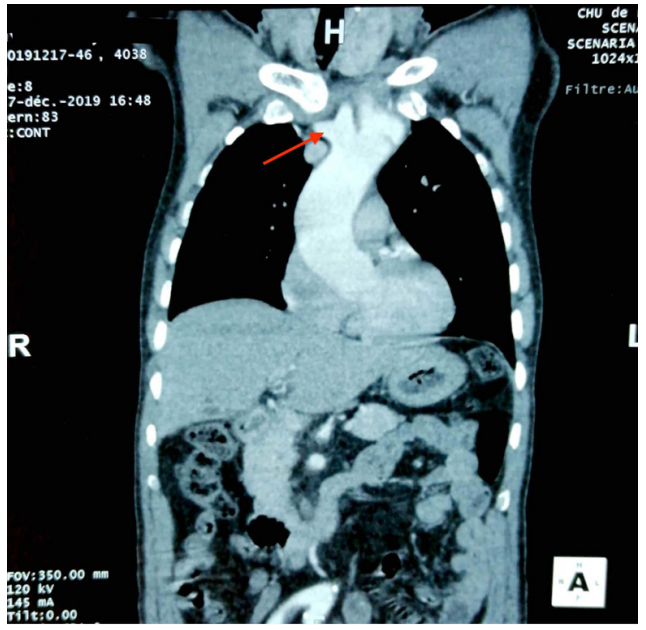
Figure 4: Thoracic angioscan (Bi-carotid trunk).

Figure 5: Thoracic angioscan (Arteria lusoria).

Figure 6: Doppler ultrasound of the renal arteries
Discussion
The aberrant right subclavian artery or arteria lusoria is the most frequent malformation of the aortic arch, its incidence is in the order of 0.5 to 2% in the general population [1]. Bayford, who gave it the name “dysphagia lusoria”, described this vascular anomaly in its fullest form in 1794 [2]. Female prevalence is higher than male in isolated forms [9]. It is during the 7th week of intrauterine development that the dorsal aorta, which remains in connection with the right 4th branchial arch, receives the right 7th cervical inter-segmental artery to form the right subclavian artery. If the right 4th branchial arch disappears or regresses instead of joining the right 7th inter-segmental cervical artery, this one joins the descending aorta crossing the midline and passing behind the esophagus [10]. The pathophysiology of this malformation remains unknown and could include a factor of hemodynamic, genetic and evolutionary origin [11]. Clinically, arteria lusoria is often asymptomatic, as the latter does not form a complete ring around the esophagus or trachea, most often it is discovered incidentally during chest exploration. Other pathologies as in the case of our patient. It becomes symptomatic essentially in three cases: on the one hand when the esophagus and the trachea are compressed between the "arteria lusoria" behind and the bi-carotid trunk in front [3], on the other hand when there is an aneurysm of this artery which constitutes a formidable complication, and finally with age during arteriosclerotic degeneration of the artery, or the occurrence of fibro-muscular dysplasia [12].
The main clinical sign is dysphagia called dysphagia lusoria, it is a dysphagia with solids. Dyspnea or chronic cough may be indicative of compression of the trachea. This clinical sign was absent in our patient. The birth of this artery is better visualized by cross-sectional imaging means, in particular the scanner and the angio-MRI. No study has been carried out in the sense of studying the sensitivity, specificity and superiority of one examination over another in the exploration of this malformation. In CT, it is about a vessel, which arises from the posterior surface of the aorta, presenting a retro- oesophageal path to go up and forward in the axillary region. If the MRI is performed, it could easily show this anomaly, in posterior coronal section, it highlights a vessel originating from the isthmus of the aorta, which has an oblique path up and to the right and which joins the axillary region. Sagittal sections show the retro esophageal location [13]. Helical CT and MRI are two competing non-invasive or minimally invasive methods in the diagnosis of aortic dissections on the one hand, and birth defects of the supra- aortic trunks on the other hand, with values for sensitivity and high specificity, between 95% and 100% [11]. No treatment is indicated for asymptomatic arteria lusoria. Treatment is only justified if it causes bothersome dysphagia or in the event of complications. There is no evidence of a higher severity of aortic-lusoria artery dissection under conservative treatment; there is no reported observation of the evolution of these dissections on this particular area [11]. In our patient, after stabilization of his symptomatology by medical treatment, a surgical indication was made.
Conclusion
Arteria lusoria is a rare, often asymptomatic vascular malformation discovered incidentally. Its diagnosis should lead the radiologist to look for abnormalities in the heart and large vessels.
References
- Zapata H, Edwards JE, Titus JL. Aberrant right subclavian artery with left aortic arch: associated cardiac anomalies. Pediatr Cardiol. 1993; 14: 159-165.
- Bayford D. An account of a singular case of deglutition. Mem Med Soc London. 1794; 2: 275-286.
- Klinkhamer AC. Aberrant right subclavian artery. Clinical and roentgen logic aspects, Am J Roentgenol Radium Ther Nucl Med. 1966; 97: 438-446.
- Akers DL Jr, Fowl RJ, Plettner J, et al. Complications of anomalous origin of the right subclavian artery: case report and review of the literature. Ann Vasc Surg. 1991; 5: 385-388.
- Chew FS, Panicek DM, Heitzman ER. Late discovery of a posttraumatic right aortic arch aneurysm. Am J Roentgenol. 1985; 145: 1001-1002.
- Mulligan S, Nath PH, Keller FS, et al. Acquired diseases of aberrant subclavian arteries. J Thorac Imaging. 1989; 4: 76-81.
- Weinberger G, Randall PA, Parker FB, et al. Involvement of an aberrant right subclavian artery in dissection of the thoracic aorta: diagnostic and therapeutic implications. Am J Roentgenol. 1977; 129: 653-655.
- Kawamoto S, Bluemke DA, Fishman EK. Aortic dissection involving an aberrant right subclavian artery: CT and MR fin- dings. J Comput Assist Tomogr. 1998; 22: 918-921.
- Molz G, Burri B. Aberrant subclavian artery (arteria lusoria): sex differences in the prevalence of various forms of the malformation. Evaluation of 1378 observations. Virchows Arch A Pathol Anat Histol. 1978; 380: 303-315.
- Papadatos D. 3 anatomical observations of a right subclavian artery originating from the aortic arch (arteria lusoria). Anat Anz. 1976; 140: 100-117.
- Lami N, Laissy JP, Gibeault M, et al. Dissection aortique intéressant une artère sous- clavière droite rétro-œsophagienne (lusoria) : aspects TDM et IRM. J Radiol. 2002; 83: 653-655.
- Gross RE, Ware PF. The surgical significance of aortic archanomalies. Surg Gynecol Obstet. 1946; 83: 435-448.
- Myers PO, Fasel JHD, Kalangos A, et al. Arteria lusoria: Developmental anatomy, clinical, radiological and surgical aspects. Ann Cardiol Angeiol. 2010; 59: 147-154.