Assessment of Maternal Left Ventricular Dysfunction and Remodeling in Gestational Hypertension
Author'(s): Ahmed Y. Nammour, Metwally Hassan El-amry, Ali Ibrahim Attia, Ahmed Abdel Mohsen Alsaghir Hegab, and Yasser Abdel Rahman*
Cardiovascular Department, Faculty of Medicine, Benha University
*Correspondence:
Yasser Abdel Rahman, Cardiovascular department, Faculty of medicine, Benha University.
Received: 20 April 2021; Accepted: 02 June 2021
Citation: Nammour AY, El-amry MH, Attia AI, et al. Assessment of Maternal Left Ventricular Dysfunction and Remodeling in Gestational Hypertension. Cardiol Vasc Res. 2021; 5(3): 1-5.
Abstract
Background: The first trimester of pregnancy is where the mother's hemodynamic adaptation starts. A raise in preload, a drop in afterload, improved conduit vessel enforcement, ventricular remodeling, and a change in the renin system cause cardiac production to increase and diastolic activity to change. -the renin-angiotensinaldosterone axis.
Aim: To assess maternal left ventricular dysfunction and remodeling in gestational hypertension.
Methods: Our study was conducted on 50 patients divided on two groups as patients and control groups each of them 25. All subjects were evaluated by history taking, clinical examination, routine laboratory investigations, 12-lead ECG and echocardiography.
Results: There was a statistically highly significant correlation between patients and control groups in age and parity with p values (0.027) and (0.023) respectively and significant correlation in left ventricular remodeling with p value for normal geometry and concentric LVH (<0.001) and (0.05) respectively. There was a significant correlation between patients and control groups with as regard left ventricular diastolic function in E/A ratio and septal E with P values <0.001 for both of them. There was a significant correlation between patients and control groups in using GLS with P value 0.001.
Conclusion: As compared to normotensive deliveries, gestational hypertension is correlated with retained left ventricular systolic activity, subclinical diastolic dysfunction, and left ventricular remodeling in the context of increased mass and wall thickness, as well as a higher prevalence of concentric remodeling. Speckle monitoring echocardiography is important in the early identification of systolic dysfunction
Keywords
Introduction
Pregnancy induces drastic, typically reversible improvements in a woman's cardiovascular system as well as changes in maternal circulation, all of which necessitate necessary modifications in order for the baby to grow naturally. As this adaptation stalls, hypertension, like pre-eclampsia, develops as a result [1].
Pre-eclampsia is a pregnancy-related condition that causes persistent hypertension, pathological edema, and proteinuria. Pre-eclampsia impacts 5% of births and causes an excessive pressure load on the heart, which can lead to a deterioration of ventricular activity. In such situations, the hemodynamic state differs from that of a typical birth, and the preeclamptic period is marked by elevated CO. Women with pre-eclampsia have distinct hemodynamic results more than women who are pregnant normally, according to cross-sectional analyses [2].
At different stages of pregnancy, normal, intensified, and depressed functions have all been registered. Many researches have shown that these significant hemodynamic modifications during breastfeeding are responsible for the occurrence of several cardiac attack signs and symptoms. In people with pre- eclampsia, these hormonal alterations may be observed as early as the first and second trimesters of pregnancy. The non-invasive procedure of echocardiography is the most effective for measuring hemodynamic status in pregnancy: The procedure is easy, fast, and painless for the patient [3].
In comparison to stable, normotensive pregnant people, echocardiographic examination of various parameters of systolic and diastolic left ventricular (LV) activity in patients with gestational hypertension (GH) showed alterations in LV function and geometry. However, the majority of these analyses compared single tests, while only one looked at improvements in these parameters over time during pregnancy and after birth. Furthermore, the conclusions are contradictory. The fact that both of these studies used standard parameters of LV systolic and diastolic function, which are based on loading conditions and contractility, could explain the disparity in performance [4].
In contrast, utilizing tissue Doppler imaging of the mitral annulus to calculate ventricular long-axis velocities (S′) and amplitude offers a more accurate index of systolic activity than LV ejection fraction (EF), which is particularly useful for detecting early systolic dysfunction induced by subclinical disease. It was also shown that it is a preload independent index of systolic feature [5].
Speckle monitoring is a newly evolved echocardiographic method for determining the degree of myocardial deformation, or pressure, during the cardiac cycle. Speckle detection is achieved in a two- dimensional echocardiographic picture by an automatic calculation of the interval between speckles in a single ventricular segment. The erratic reflection of ultrasound, which can be monitored during the cardiac cycle, causes speckles. It is angle-independent and less vulnerable to operator-related measuring mistakes since it is built on observing the trajectory of a speckle of the picture over time in relation to its original position. Speckle monitoring enables longitudinal, lateral, and circumferential pressure to be measured, which has been used to predict improvements in left ventricular activity and geometry [6].
Strain is a measurement of an object's deformation due to the original structure, represented as a percentage change from the original dimension. The variation in distance and velocity of the speckle during the cardiac period is used to measure strain using speckle monitoring. Positive numbers indicate lengthening, whereas negative numbers indicate contraction. Cardiac arrest Myofibrils have a helical nature and they may be oriented in the radial, circumferential, and longitudinal planes. Unlike left ventricular ejection fraction, which is a global metric, strain with speckle monitoring assesses both regional and global function while also identifying the affected myocyte population. Furthermore, the left ventricular ejection fraction equation allows geometric predictions that speckle monitoring does not [7].
The aim of this research was to compare the diastolic and systolic functions as well as the left ventricular geometric pattern in pregnant women with gestational hypertension to pregnant women with normal blood pressure.
Patients and Methods
This study was carried out at Benha university hospitals from November 2019 to January 2021 on 50 patients diagnosed as gestational hypertension. The patients were divided into 2 groups: Group A: 25 pregnant patients diagnosed as gestational hypertension, Group B: 25 pregnant patients with normal blood pressure during pregnancy.
Inclusion criteria
Confirmed diagnosis of gestational hypertension for the first time as recommended by the European society of cardiology in 2018 by clinical presentation as persistent elevation of arterial blood pressure over 140/90 starting from 20 weeks of last menstrual period till full term with or without proteinuria [8].
Exclusion criteria
- Patients were unlikely to cooperate in the study or unwillingness to give informed consent.
- Chronic hypertensive patients.
- Patients who developed
- Tobacco and alcohol use.
- History of heart disease as ischemic, valvular and congenital heart disease.
- Preexisting chronic medical problem as diabetes mellitus, renal, hepatic and connective tissue disease.
- Undetermined time of development of hypertensive
- Hepatitis (c) positive
The test group followed the same inclusion and exclusion requirements, but did not meet the concept of hypertension. Both monitors had a standard electrocardiogram to rule out any potential sources of interference.
All patients were subjected to history taking, clinical examination and Investigations as
- Electrocardiogram (ECG); To assess strain pattern of hypertension and left ventricle hypertrophy, Old ischemic changes, Rhythm abnormalities, Rate and QRS duration
- Laboratory investigation: Urine analysis, Complete blood count, Liver function test, Electrolytes, BUN, creatinine, and Random blood sugar
- Echocardiography
- Standard 2-dimensional (2D) and strain echocardiography were performed on all subjects while lying in the left lateral decubitus position using a 3.5-MHz.
- Systolic function was detected using Simpson
- Measurements of the thickness of interventricular septum and posterior wall, and the diameter of LV cavity were
- The LV geometries were classified into 4 groups based on left ventricle mass index (LVMI) (61 ± 8 g/m(2) in women) and relative wall thickness (RWT) (0.22-0.42) as the following:
- Normal geometry: if LVMI and RWT were less than the mean of those corresponding to normotensive pregnant women (NPW).
- Concentric hypertrophy (CH): if both LVMI and RWT were increased.
- Eccentric hypertrophy (EH): if LVMI was increased and RWT was normal.
- Concentric remodeling (CR): if LVMI was normal and RWT was increased.
- Pulsed wave Doppler of transmitral LV inflow was performed in the apical 4-Chamber view with the sample volume placed at the level of the mitral valve tips and Doppler variables were analyzed during 3 consecutive The following measurements of global LV diastolic function were determined:
- Peak early (E) and late (A) diastolic mitral flow velocity and their ratio E/A, early (Ea) diastolic mitral annular velocity, deceleration time of the E wave and LV isovolumetric relaxation time (IVRT).
- Doppler time intervals were measured from mitral inflow and LV outflow velocity time intervals and the index of combined LV systolic and diastolic function (the sum of isovolumetric contraction time [ICT] and IVRT divided by ejection time) was
- Tissue Doppler technique was used to measure the velocity of movement of septal and lateral aspects of the mitral annulus. The myocardial velocities have three main components: systolic wave (s´), early diastolic (e´) and late diastolic wave (a´). Septal e´ <8 cm/s and/or lateral e´<10cm/s suggests the presence of diastolic
- Two-dimensional speckle tracking echocardiography (2D STE): Longitudinal strain rate was assessed in the 6 LV walls and the software algorithm automatically segments the LV into 18 equidistant segments and each segment is analyzed
Statistical analysis
Using Microsoft Excel program, data from the past, simple clinical analysis, laboratory investigations, and measured echocardiographic measurements were entered. IBM SPSS program version 20.0 was used to interpret the data that was fed into the device. (IBM Corporation, Armonk, NY). Number and percent were used to represent qualitative results. The Kolmogorov-Smirnov test was used to ensure that the distribution of variables was natural. Scale (minimum and maximum), mean, standard deviation, median, and interquartile range were used to characterize quantitative results (IQR). The significance of the obtained findings was assessed at a 5% stage. For abnormally distributed quantitative variables, the Mann Whitney test was used to compare two classes, while the Kruskal-Wallis test was used to measure the difference between the medians of more than two groups for non-parametric statistics. For naturally distributed quantitative variables, the F-test (ANOVA) was used to evaluate more than two classes. The significance of the collected findings was assessed at a 5% degree of significance.
Ethical consideration
Both patients were given the opportunity to give their informed consent. The Institutional Review Board (IRB) of Benha University's faculty of medicine gave its approval to the report. There are no conflicts of interest between the nominee and either of his or her supervisors.
Results
The study was done on 50 pregnant women as control and patient groups aged from 18 to 35 years old with the mean age 30 for case group and 27 years for control group. There were significant differences between both groups as regarding age and parity with p values (0.027) and (0.023) respectively. There were significant differences in SBP between both groups with P values <0.001. There were significant differences in DBP between control and patient groups with P value <0.001. There were no significant differences in heart rate between both groups with P value 0.09 (Table 1).
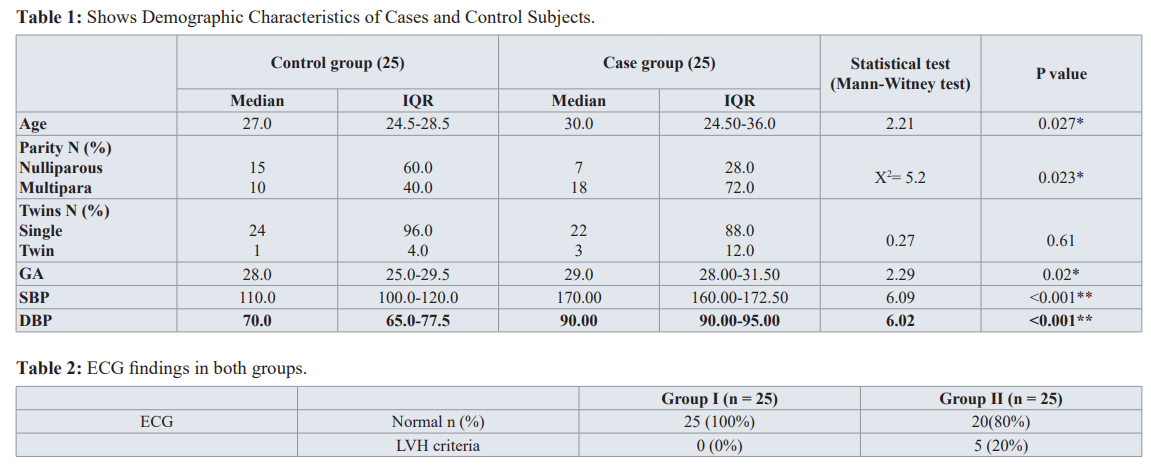
There were significant differences left ventricular hypertrophy criteria between both groups as regard ECG findings. (P value = 0.05), Table 2.
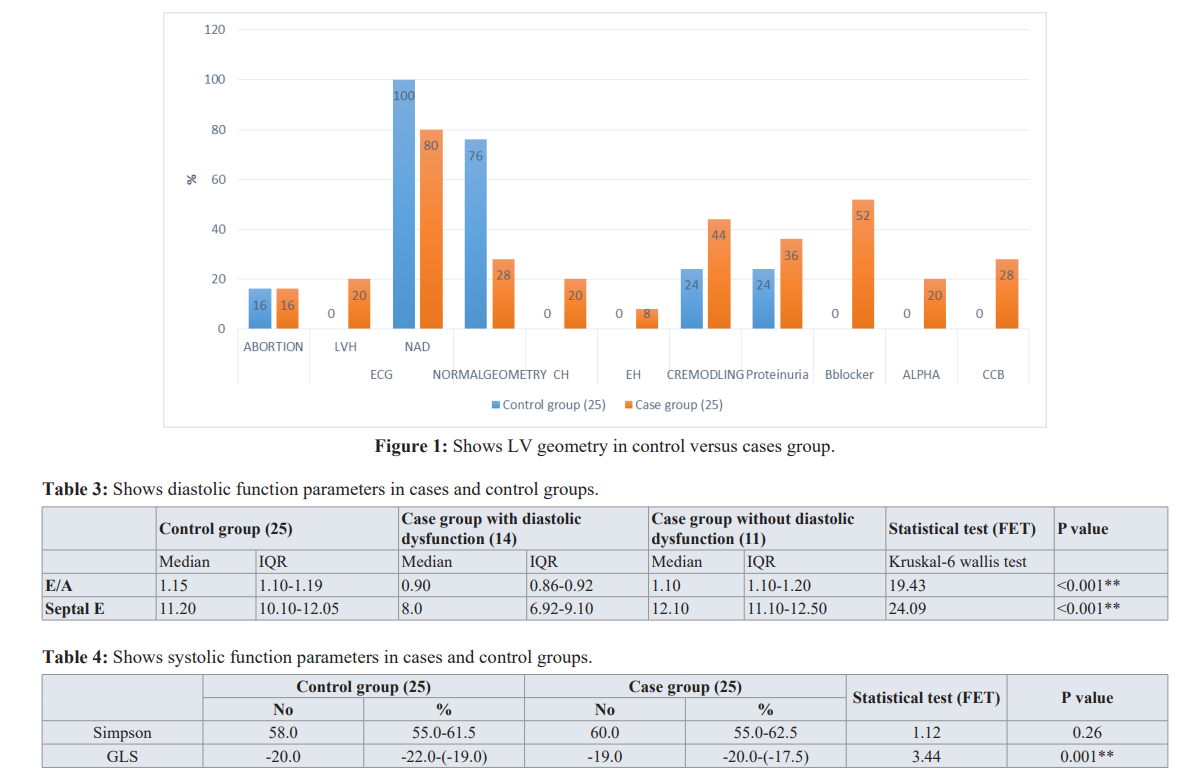
There were significant differences in normal geometric and concentric LVH pattern between both groups with P value <0.001 and 0.05 respectively. There were no significant differences between both groups as regard eccentric hypertrophy and concentric remodeling with P values 0.5 and 0.14 respectively (Figure 1).
There were significant differences in E/A ratio between both groups with P value 0.01 but no significant difference as regard to septal E with P value 0.09. LVESV % change showed no significant difference between both groups with P value = 0.556, Table 3.
There were no significant differences in ejection fraction by Simpson method between both groups with P value 0.26. But with GLS speckle tracking technique there were significant difference between both groups with P value 0.001, Table 4.
Discussion
In this study, we used 2D, Simpson and pulsed wave Doppler and tissue Doppler and GLS speckle tracking to compare the left ventricular function and remodeling in the two groups.
This study demonstrated that there were significant difference in normal geometry with p value <0.001 and concentric hypertrophy with p value 0.05 but there were no significant difference in eccentric hypertrophy and concentric remodeling between the two groups with p value 0.5 and 0.14 respectively.
In Herbert Valensise et al, [9] exhibited In the normotensive population, 80.95 percent (17 of 21) of the subjects had a regular geometric pattern; in the hypertensive group, 19.05 percent (4 of 21) of the subjects had an altered geometric pattern, with two having concentric remodeling and two having eccentric hypertrophy.
In the hypertensive population, 100% of the patients have an altered graphical pattern, with concentric remodeling accounting for 28.57 percent (6 of 21), eccentric hypertrophy accounting for 38.10 percent (8 of 21), and concentric hypertrophy accounting for 33.33 percent (7 of 21). The proportion of participants with left ventricular geometric alterations was slightly higher in the hypertensive community than in the control group (100 percent vs 19.05 percent P0.001).
In Karen melchiorre et al, [10], the proportion of patients with LV geometric remodeling was slightly higher in the PE community (36 of 50 [72 percent]) compared to the control group (12 of 50 [24 percent]; P0.0001; There were ten cases of LV concentric hypertrophy among PE patients. The development of a basal septal bulge (n=7) was only seen in the women with PE who also had global diastolic dysfunction (P=0.001).
In terms of diastolic activity, this analysis found a major difference in E/A ratio and septal E, all of which had a P value of 0.001.
In Mi-Jeong Kim.et al, [11] By comparing hypertensive and normotensive people, diastolic functional parameters were slightly lower in hypertensive women. Hypertensive women have a somewhat lower E/A ratio (1.4 0.4 vs. 1.1 0.3, p = 0.001) and e' velocity (9.2 2.2 vs. 7.9 2.4, p = 0.001). Hypertensive women had significantly higher peak A wave velocity (62 15 vs. 75 16, p 0.001) and E/e' ratio (9.2 2.5 vs. 11.0 3.0, p 0.001).
In James S. Castleman.et al, [12] The E/A ratio decreases toward term in regular pregnancy, according to many reports. In GH, there is a larger decrease in E/A than in pregnancy without hypertension. Diastolic activity is often harmed in pre-eclampsia, where the normal E/A ratio is exaggerated. In five trials, the ratio of early diastolic mitral inflow velocity to early diastolic mitral annular velocity (E/e′) was substantially higher in pre-eclamptic women, implying higher LV filling pressures. E/e′ was shown to be slightly higher in an early-onset pre-eclampsia subgroup than in a late-onset pre-eclampsia subgroup. 40 Diastolic dysfunctions were seen in 40% of pregnancies complicated by pre-eclampsia at term, relative to 14% of controls, in an analysis that used a composite of diastolic indices to detect diastolic dysfunction. 45 Diastolic instability was present at 20 to 23 weeks in women who experienced preterm pre-eclampsia, but not in women who developed pre-eclampsia at term, according to another report. Despite data that left atrial mechanical activity is comparable in pre-eclampsia and normotensive pregnant controls, diastolic dysfunction is more prominent in cases consistent with fetal growth restraint.
As regard to systolic function This study demonstrated that there were significant difference in GLS speckle tracking values between control and patients groups with P value <0.001 but showed non- significant difference by Simpson method with p value 0.26.
Conclusion
As compared to normotensive deliveries, gestational hypertension is correlated with retained left ventricular systolic activity, subclinical diastolic dysfunction, and left ventricular remodeling in the context of increased mass and wall thickness, as well as a higher prevalence of concentric remodeling. Speckle monitoring echocardiography is important in the early identification of systolic dysfunction.
Limitations
One limitation is the relatively small sample size so further studies are recommended to be conducted over a larger sample size for more accurate results, another limitation is that follow up of cardiac function after delivery was not performed.
References
- Soma-Pillay P, Catherine NP, Tolppanen H, et Physiological changes in pregnancy. Cardiovasc J Afr. 2016; 27: 89-94.
- Solanki R, Maitra Echocardiographic assessment of cardiovascular hemodynamics in preeclampsia. J Obstet Gynecol India. 2011; 61: 519-522.
- Tangeda P, Shastri N. Maternal left ventricular systolic and diastolic function during second trimester of pregnancy with J Dr NTR Univ Heal Sci. 2015; 4: 224-228.
- Yuan L, Duan Y, Cao Echocardiographic study of cardiac morphological and functional changes before and after parturition in pregnancy -induced hypertension. Echocardiography. 2006; 23: 177-182.
- Correale M, Totaro A, Ieva R, et Tissue Doppler imaging in coronary artery diseases and heart failure. Curr Cardiol Rev. 2012; 8: 43-53.
- Mondillo S, Galderisi M, Mele D, et al. Speckle -tracking echocardiography: a new technique for assessing myocardial J Ultrasound Med. 2011; 30: 71-83.
- Shahul S, Rhee J, Hacker MR, et Subclinical left ventricular dysfunction in preeclamptic women with preserved left ventricular ejection fraction: a 2D speckle-tracking imaging study. Circ Cardiovasc Imaging. 2012; 5: 734-739.
- Sibai Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003; 102: 181-192.
- Valensise H, Novelli GP, Vasapollo B, et Maternal diastolic dysfunction and left ventricular geometry in gestational hypertension. Hypertension. 2001; 37: 1209-1215.
- Melchiorre K, Sharma R, Thilaganathan B. Cardiovascular implications in preeclampsia: an Circulation. 2014; 130: 703-714.
- Kim MJ, Seo J, Cho KI, et al. Echocardiographic assessment of structural and hemodynamic changes in hypertension- related J Cardiovasc Ultrasound. 2016; 24: 28-34.
- Castleman JS, Ganapathy R, Taki F, et al. Echocardiographic structure and function in hypertensive disorders of pregnancy: a systematic Circ Cardiovasc Imaging. 2016; 9: e004888.