Assessment of Oral Health of Valvular Heart Diseases Patients in The University Hospital Mother-Children le Luxembourg (UH-MCL) in Bamako
Author(s): Maiga Asmaou Kéita1, Bâ Hamidou Oumar2*, Ba Boubacar3, Sangaré Ibrahima2, Camara Youssouf4, Sidibé Noumou2, Touré Mamadou2, Coulibaly Souleymane5, Sidibé Samba5, Konaté Massama5, Doumbia Coumba Thiam4, Sonfo Boubacar4, Diakité Mamadou5, Menta Ichaka1, Diall Ilo Bella5, Bâ Ahmed3 and Diarra Mamadou Bocary1
1University Hospital Mother-Children Le Luxembourg, Cardiology, Bamako, Mali.
2University Hospital Gabriel Touré, Cardiology, Bamako, Mali.
3University Hospital Odontostomatology, Bamako, Mali.
4University Hospital Bocar Sidy Sall, Cardiology, Kati, Mali.
5University Hospital Point G, Cardiology, Bamako, Mali.
*Correspondence:
Bâ Hamidou Oumar, University Hospital Gabriel Touré, Cardiology, Bamako, Mali.
Received: 29 November 2019; Accepted: 22 December 2019
Citation: Maiga Asmaou Kéita, Bâ Hamidou Oumar, Ba Boubacar, et al. Assessment of Oral Health of Valvular Heart Diseases Patients in The University Hospital Mother-Children le Luxembourg (UH-MCL) in Bamako. Cardiol Vasc Res. 2019; 3(5); 1-5.
Abstract
Introduction: Oral hygiene is particularly important in patients with valvular heart disease because of the risk of infective endocarditis. The lack of published data on oral hygiene in Mali on the subject motivated this study to assess the oral status of patients with valvular diseases at the University Hospital Mother Child Le Luxembourg (UH-MCL).
Methodology: This was a cross-sectional and descriptive study based on observation of the oral status of 100 patients with valvulopathy. The study took place from May to September 2017 at UH-MCL. Was included any patient seen in consultation, suffering from valvulopathy and giving their consent to answer the questionnaire and to be examined by an dental practioner. The interview and oral examination data were collected on a survey formulary, data entry and analysis performed with the Epi Info 3.5.3 French version. All included patients gave their verbal consent and the confidentiality of the data was respected by making the formulary anonymous.
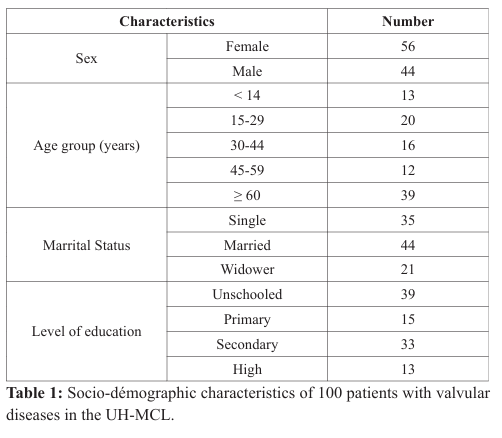
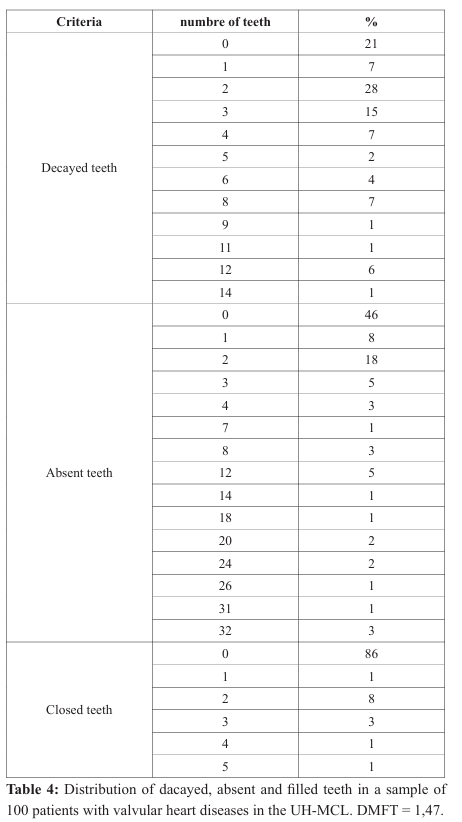
Results: Mean age of the sample was 45.6. Female and those over 60 years made respectively 56 % and 39% of the sample. Unschooled patients represented 39% of the sample. Arterial hypertension was found in 31% of patients. The quality of oral hygiene was rated as acceptable and poor in respectively 51% and 39% of all cases. The daily brushing frequency of 2 and the type of modern toothbrush were found respectively in 56% and 66% of cases. The brushing technique was found to be bad in 75% of cases and 83% of brushing was done before breakfast, 50% after dinner. Plate and gingival indices were 55% and 78%, respectively, for plate 1 and gingival index 1 The oral diseases were dominated by halitosis (14%), dental mobility (10%) and dental prosthesis mobility (8%). The dental state was estimated with a DFMT index of 1.47, deduced from the condition of the teeth. The proportion of decayed, absent or occluded teeth was 79%, 54% and 14%, respectively (Table 4).
Conclusion: There is a need to further promote oral health particularly in patients with heart diseases, necessitating a multidisciplinary and multsector collaboration.
Keywords
Introduction
Oral hygiene, Valvulopathies, Outpatients, Bamako.heart disease because of the risk of infective endocarditis (IE) [1] and oral sphere is entry point for IE in 22% of known entry [2]. Patients with cardiovascular disease (CVD) are often referred to the dental office for oral care that can be invasive and can affect their health [3-5].
Classically the most common etiology of valvulopathy is acute rheumatic fever (ARF). In most high income countries (HIC), prophylaxis and antibiotic therapy have eliminated the risk of rheumatic heart diseases (RHD) in favor of degenerative etiology and non-rheumatic endocarditis [6,7]. Studies have linked infectious endocarditis to oral diseases [2]. this is not the case in low income countries (LIC), inclusive ours.
The oral state of patients with rheumatic valvulopathy requires management according to a multidisciplinary and adequate treatment plan to improve their general health and quality of life. The lack of studies in Mali on the subject motivated this study to assess the oral status of patients with valvular diseases at the University Hospital Mother Child Le Luxembourg (UH-MCL). The assessment of dental and periodontal treatment needs will contribute significantly to improve the health of the heart patients in Mali.
Methodology
This was a cross-sectional and descriptive study based on observation of the oral status of patients with valvulopathy. The study took place from May to September 2017 at UH-MCL. Was included any patient seen in consultation, suffering from valvulopathy and giving their consent to answer the questionnaire and to be examined by a dental practionner. For the oral examination, the material consisted of: a sterile tray with a probe, dental mirror, tweezers, rolls of cottons, sterile compresses, gloves and masks.
Definition of terms
Education level has been categorized according to years spent in school as: - Unschooled: 0
- Primary: 1-9
- Secondary: 10-12 - High: > 12
Oral hygiene was assessment as
Good: Visible lack of dental plaque with naked eyes, unloaded tongue and acceptable breath Acceptable: minimal plaque, slightly loaded tongue and acceptable breath Bad: presence of dental plaque visible to the naked eye, loaded tongue and halitosis.
The interview and oral examination data were collected on a survey formulary, data entry and analysis performed with the Epi Info 3.5.3 French version. All included patients gave their verbal consent and the confidentiality of the data was respected by making the formulary anonymous.
Results
One hundred patients with a mean age of 45.6 [8-99], 56 female patients were consecutively registered. Patients over 60 years made 39% and those married 44% of the sample. Unschooled patients represented 39% of the sample (Table 1).
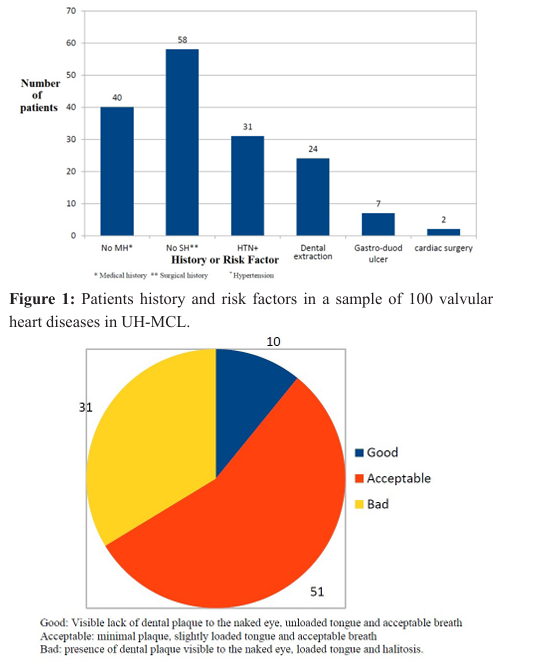
Arterial hypertension was found in 31% of patients. Proportions of 40% and 58% of the patients had respectively nor medical neither surgical history (Figure 1).
The quality of oral hygiene was rated as acceptable and poor in respectively 51% and 39% of all cases (Figure 2).
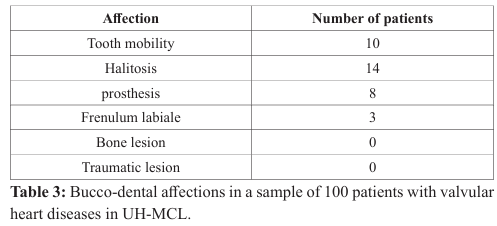
The daily brushing frequency of 2 and the type of modern toothbrush were found respectively in 56% and 66% of cases. The brushing technique was found to be bad in 75% of cases and 83% of brushing was done before breakfast, 50% after dinner (Table 2).
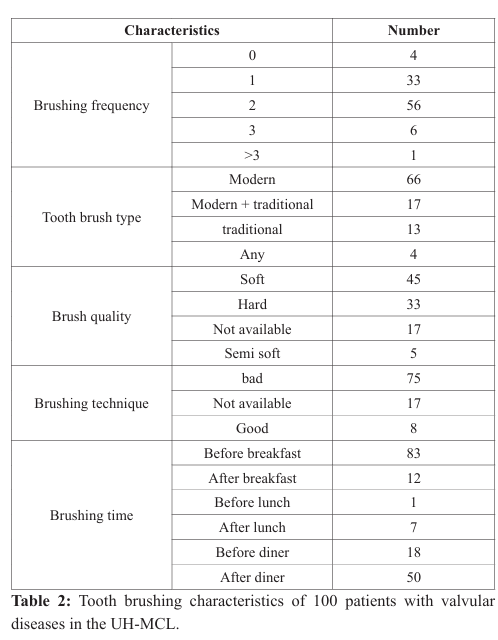
Plate and gingival indices were 55% and 78%, respectively, for plate 1 and gingival index 1 The oral diseases were dominated by halitosis (14%), dental mobility (10%) and dental prosthesis mobility (8%) (Table 3).
The dental state was estimated with a DMFT index of 1.47, deduced from the condition of the teeth. The proportion of decayed, absent or occluded teeth was 79%, 54% and 14%, respectively (Table 4).
Discussion
Our sample with mitral and / or aortic valvulopathies was composed of 56% of female patients. This female predominance in consultation observed in several previous studies has not yet found a satisfactory explanation. May be could women consult earlier than men? This female predominance was not found by Iung [6].
Hypertension (HTN) was the most common cardiovascular risk factor in 31%, concordant with studies giving a prevalence of HTN of nearly a quarter of the general population [8]. Hypertension and periodontitis are linked together and could potentiate each other [9]. The most represented age group of 60 and more in our sample was different for Diop in Dakar (Senegal) [10] with lower proportions (12.3%) and in the URCAM study with 74% [2], probably related to the choice of the sample.
Unschooled patients represented the majority in our sample, reflecting the low level of development as in most developing countries. The frequency of brushing at least twice a day and the use of the modern toothbrush seem to be well established and reflect a higher degree of information in this direction. On the other hand, there is a deficit in the brushing technique, which in the majority of cases is bad and reflects a deficit at this level, hence the intensification of information efforts at different levels to apply good technical brushing practices..
The oral hygiene considered bad in 39% of the cases in our study is slightly higher than data published by Fanjeaux with 33% [11] but clearly lower than those of Gandega with 77.12% in the University Dentistry Center (UDC) [12]. One explanation might be that the UDC as specialized facility receives patients with more severe conditions and / or advanced stages of diseases. The overall incidence of caries was higher in our sample (79%), contrary to URCAM data , with 36% [2] probably due to the higher frequency of dental consultations in developed countries. On the other hand, our sample found significantly fewer closed teeth (14%) compared to the results of the URCAM study (70%).
The plaque index 1 (55%) is higher than that of Diop with 33.3% of cases and the gingival index 1 (78%) similar to the results of Diop [10].
The DMFT evaluating the caries experience was 1.47 in our sample and it is known that this index is very variable according to various conditions [13-15]. Our index appears relatively high particularly in this population of patients with valvular heart diseases. Promoting oral care specially among patients with valvulopathies is a must as regular dental visits in e.g once a year for professional cleaning has been found to reduce CVR by 14 [16].
Limitations
It was not possible to evaluate the oral status based on the type of valve involvement in this study, which opens the way to the next step which should focus on oral status by type of valvulopathy and generally by type of cardiac involvement.
Conclusion
Regular dental visit has to be promoted particularly in patients with heart diseases as these 2 conditions are mutually aggravating factors leading to serious even life threatening conditions. A colloboration of general practionner, dental practionner at health system level and educators at education level are necessary to improve oral health.
References
- Millot S, Lesclous P, Colombier ML, et al. Position paper for the evaluation and management of oral status in patients with valvular disease: Groupe de Travail Valvulopathies de la Société Française de Cardiologie, Société Française de Chirurgie Orale, Société Française de Parodontologie et d’Implantologie Orale, Société Française d’Endodontie et Société de Pathologie Infectieuse de Langue Française. Arch Cardiovasc Dis. 2017; 110: 482-494.
- Endocardite infectieuse et état bucco-dentaire. http://www.orspoitou-charentes.org/pdf/Endocardite-URCAM.pdf
- Minkle Gulati, Vishal Anand, Nikil Jain, et al. Essentials of Periodontal Medicine in Preventive Medicine. 2013; 4: 988-994.
- Bhateja S. High prevalence of cardiovascular diseases among other medically compromised conditions in dental patients: A retrospective study. J Cardiovasc Dis Res. 2012; 3: 113-116.
- Schwahn C, Polzer I, Haring R, et al. Missing, unreplaced teeth and risk of all-cause and cardiovascular mortality. Int J Cardiol. 2013; 167: 1430-1437.
- Iung B. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003; 24: 1231-1243.
- Le Bot A, Jégo P, Donal E, et al. Les endocardites non infectieuses. Rev Médecine Interne. 2018; 39: 782-791.
- Bâ HO, Camara Y, Menta I, et al. Hypertension and Associated Factors in Rural and Urban Areas Mali: Data from the STEP 2013 Survey. Int J Hypertens. 2018; 2018: 1-7.
- Tsioufis C, Kasiakogias A, Thomopoulos C, et al. Periodontitis and blood pressure: The concept of dental hypertension. Atherosclerosis. 2011; 219: 1-9.
- Diop O. Etat parodontal et affections cardiovasculaires (à propos d’une étude cas-témoins portant sur 169 sujets à la clinique de cardiologie de l’hôpital Aristide le Dantec). Available from: http://bibnum.ucad.sn/viewer.php?c=thm&d=THM-46363
- Fanjeaux N Nicolas Fanjeaux. Endocardite infectieuse d’origine dentaire: mythe et réalités. Sciences du Vivant [q-bio]. 2014. hal-01733771. Available from: https://hal.univ-lorraine.fr/hal01733771/document
- Gandega S. Les maladies parodontales au Centre Hospitalier Universitaire d’Odontostomatologie de Bamako: A propos de 153 cas. 2013; 111). Available from: http://www.keneya.net/fmpos/theses/2013/med/pdf/13M214.pdf.
- Tanaka MH, Bocardi K, Kishimoto KY, et al. DMFT index assessment and microbiological analysis of Streptococcus mutans in institutionalized patients with special needs. Brazilian Journal of Oral Sciences. 2009; 8: 9-13.
- JO García-Cortés JP Loyola-Rodriguez A Loyola-Leyva, et al. Socio-behavioral Factors Associated to Caries Prevalence and DMFT Index in Adolescents and Young Adults in a Developing Country. 2017.
- RadiÄ? M, Benjak T, DeckoviÄ? Vukres V, et al. Presentation of DMF Index in Croatia and Europe. Acta Stomatol Croat. 2015; 49: 275-284.
- Park SY, Kim SH, Kang SH, et al. Improved oral hygiene care attenuates the cardiovascular risk of oral health disease: a population-based study from Korea. Eur Heart J. 2019; 40: 11381145.