Assessment of Physicians' Knowledge of the Management of Sudden Cardiac Arrest
Author(s): Dioum M*s, Wane O, Gaye C, Manga S.J., Badredine A., Ralaizandry U.S, Bindia D, Traore M.M and Mbaye A
Cardiology Department, Teaching hospital of Fann, Dakar, Sénégal.
*Correspondence:
Momar DIOUM, Cardiology Department, Teaching hospital of Fann, Dakar, Sénégal. Fax: 00221776551883.
Received: 03 Jan 2021; Accepted: 07 Feb 2022; Published: 12 Feb 2022
Citation: Dioum M, Wane O, Gaye C, et al. Assessment of Physicians' Knowledge of the Management of Sudden Cardiac Arrest. Cardiol Vasc Res. 2022; 6(1): 1-3.
Abstract
Introduction: Sudden cardiac arrest (SCA) is the abrupt loss of heart function and breathing. It is an absolute medical emergency. The management is based on the principle of the chain of survival. The main objective of this study was to assess the diagnostic and therapeutic abilities of physicians on the care of SCA.
Material And Method: It was a multicentre, cross-sectional and descriptive analytical study covering the period from September 01st, 2018 to February 30, 2019. Included were all general practitioners, emergency physicians, cardiologists and anesthetists-resuscitators who agreed to complete the survey. The parameters studied were recognition of signs of SCA and the knowledge about the steps of the chain of survival.
Results: We included 78 physicians with an average age of 35,16 years. There were 39 generalists and 39 specialists. The three SCA diagnostic criteria were known to 49 physicians (62.8%). More than half of physicians (n = 54, 69.2%) mastered the chronology of the steps of the chain of survival. The rhythm sequence of chest compressions and insufflations was controlled by 56.4% of physicians (n = 44). About the defibrillation, 70,51% (n=55) responded that it was not systematic in front of any SCA. Thirty-eight physicians were aware of the sequence of adrenaline administration. Only 24 doctors knew the time for amiodarone administration. A minority of 10 physicians has been able to fully define the acronym ABCDE.
Conclusion: The level of physicans knowledge on the management of sudden cardiac arrest is relatively average. Every physician must be trained in basic cardiopulmonary resuscitation in order to save lives.
Keywords
Introduction
Sudden cardiac arrest (SCA) is defined as the sudden interruption of heart function and breathing. This is an absolute medical emergency. Sudden cardiac arrest, or sudden cardiac death of adults, remains a major public health problem in developed and developing countries. It involves more than 600 000 deaths annually worldwide [1]. It represents the most extreme of emergencies and has not been considered irreversible since 1960, when basic cardiopulmonary resuscitation (CPR) was defined. However, the prognosis remains poor with an overall survival rate of 1.4%. There is a risk of neurological sequelae with varying degrees of consequences of cerebral hypoxia [2].
The mannagement is based on the principle of the chain of survival, proposed in 1992 by the American Heart Association (AHA) and the European Resuscitation Council (ERC), composed of 4 interdependent links with the recognition of cardiac arrest and the immediate alert by the witness(es), early cardiac chest compression, defibrillation and specialized care by the Mobile Emergency and Resuscitation Service (SMUR) team [3,4]. The first 2 survival links are for the general public and require knowledge of emergency measures and actions to be undertaken as soon as the SCA is recognized. The third link, early defibrillation, can also be performed by the witnesses. The fourth and last link of this chain is reserved for medical assistance (Emergency medical service or EMS, firefighters and SMUR) whose objective is to bring on-site the drug therapy of resuscitation.
The main objective of this study was to assess the diagnostic and therapeutic abilities of physicians on the management of SCA.
Materials and Method
It was a multicentre, cross-sectional and descriptive study with an analytical aim carried out over a period of 7 months (September 01, 2018 to February 30, 2019). Included were all general practitioners, emergency physicians, cardiologists and anesthesiologists/ resuscitators who agreed to complete the questionnaire. For this, an anonymous questionnaire was given to all the doctors immediately recovered after being completed. The parameters studied were recognition of the signs of SCA (no detectable pulse, loss of consciousnness and no breathing or agonal breathing) and knowledge of the different steps of the survival chain (recognition of cardiac arrest and immediate alert by witness(es), early chest compression, defibrillation and specialized care by the EMS team).
The data was entered with the Epi Info7® software and the analysis done with the Excel 2019® and XLSTAT-Biomed® software.
The protocol was submitted to the Scientific Ethics and Health
Research Committee of the Cheikh Anta Diop University of Dakar.
Results
We included 78 physicians with an average age of 35,16 with extremes of 28 – 62 years. There were 39 generalists and 39 specialists, including 14 anesthetists-resuscitators, 14 cardiologists and 11 emergency physicians.
The three SCA diagnostic criteria were known to 49 physicians (62,8%). Overall, 60.2% (n=47) of physicians were familiar with methods of checking for consciousness, 97.4% (n=76) checked the respiratory status, and 46,1% (n=36) appreciated heartbeats.
More than half of physicians (n = 54; 69,2%) mastered the chronology of the stages of the survival chain. The vast majority (84%) immediately alerted rescuers after recognition of cardiac arrest. The Emergency Medical Service (EMS) number (15 15) was cited by 73% of them. The numbers of SOS doctors and firefighters were cited by 21% and 15,1% respectively.
The rhythm sequence of chest compressions and insufflation was controlled by 56,4% of physicians (n = 44). The frequency of chest compressions was known to 46,1% of physicians (n=36) and the region of chest compressions by 56.4% of physicians (n=44). Almost all physicians interviewed (n=70; 89,7%) had chosen mouth-to-mouth as an insufflation technique.
For defibrillation, indications were known to 70,5% (n=55) of physicians. As for the minimum energy level of the first external electric shock, they were known to 27 doctors or 34,6%.
Thirty-eight physicians were aware of the sequence of administration of adrenaline in cases of shocking or not.
Only 24 physicians were aware of the timing of administration of amiodarone after the third external electric shock.
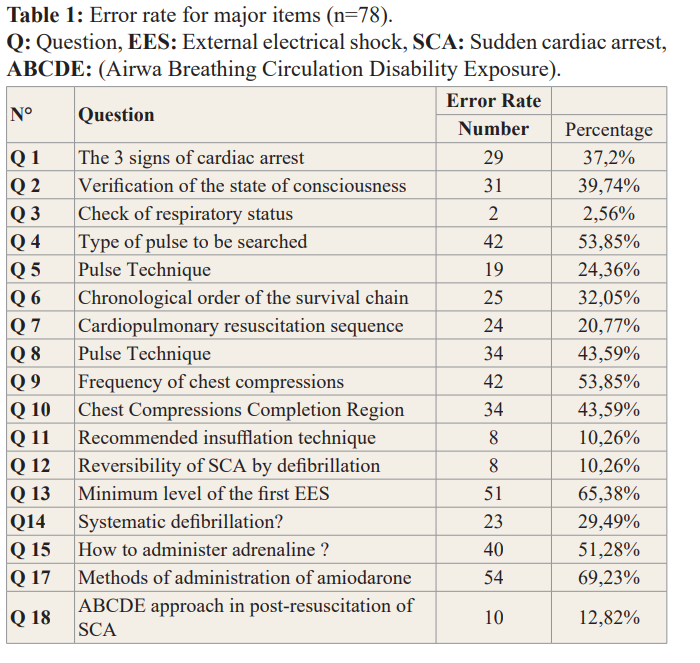
Regarding the acronym ABCDE, 39 physicians (50%) were able to explain the first 3 actions (ABCs), 7 physicians (7,6%) were unable to define the acronym D and 16 physicians (20,51%) were unable to define the acronym E. Only 10 physicians were able to fully determine the acronym ABCDE. The Error Rates for the main items are summarized in Table 1.
Discussion
Regarding the recognition of cardiac arrest, we found an inability to cite the 3 diagnostic criteria of SCA by 42,1% of generalists. This value was lower than those reported by C. Counillon [5], B. Demailly [6] and E. Cwicklinski [7] who found 72%, 74% and 69% respectively. Compared to specialists, this value was 15,3% lower. C. Gallois [8] found a value close to 33%. These results show a low level of knowledge of physicians especially generalists for SCA recognition.
The chronological order of execution of the links in the survival chain was unknown to 31% of doctors. This has a negative impact on the prognosis.
It was very satisfying and reassuring to see that the vast majority (84%) kept the reflex to alert the rescue immediately after recognition of the cardiac arrest. The EMS (15%) was quoted, alone or in association with another number, by 73% of them. SOS doctors and firefighters were cited by 21% and 15.1% respectively. In comparison, Roger et al. [9] found very similar results: 87% called paramedics, 13% called SOS doctors and firefighters. The EMS then appeared to be the reference in the emergency alert.
The rhythm sequence of chest compressions and breaths was controlled by 56,4% of physicians. E. Cwicklinski [7] had a higher rate of 75%. This shows the need for ongoing training of our doctors.
In the defibrillation knowledge assessment, our results showed that the majority of physicians knew that defibrillation is not systematic for any cardiac arrest (71%). However, they also showed that there was a real lack of knowledge about the minimum energy level to be delivered during the first external electric shock: only 35% knew that it varies between 150 and 200 joules for the semi-automatic defibrillator.
Regarding specialized resuscitation, 67% of generalists were unaware of how to administer adrenaline, compared with 35,6% in the Pyrenean study [10]. The place of adrenaline in the SCA management algorithm is well defined: as soon as possible in the case of a non-shockable rhythm and delayed in the case of a shockable rhythm [11].
Similarly, injecting amiodarone only from the 3rd external electrical schock seemed to be assimilated by 30.7% of doctors. These figures seemed alarming to us. The components of the specialized resuscitation ABCDE scheme could only be defined by ten physicians. This rate is very low. Specialized cardiopulmonary resuscitation training will need to be improved to optimize cardiological and neurological prognosis.
Conclusion
The level of physician knowledge on the management of cardiac arrest is relatively average. Therefore, any physician must be trained in basic cardiopulmonary resuscitation actions in order to save lives. This involves the organisation of continuing medical training and the establishment of well-codified protocols.
References
- Christie Atwood, Mickey S Eisenberg, Johan Herlitz, et al. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation. 2005; 67: 75-80.
- Geri G, Mongardon N, Daviaud F, et al. Neurological consequences of cardiac arrest: Where do we stand? Ann Fr Anesth Reanim. 2014; 33: 98-101.
- Truhlág A, Deakin CD, Soar J, et al. European resuscitation council guidelines for resuscitation 2015: section 4. Cardiac arrest in special circumstances. Resuscitation. 2015; 95: 148-201.
- Cummins RO, Chamberlain DA, Abramson NS, et al. Recommended guidelines for uniform reporting of data from out-of hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation. 1991; 84: 960-975.
- Camille COUNILLON TITRE. Évaluation des besoins de formation en médecine générale sur la prise en charge de l’arrêt cardiaque : une étude épidémiologique descriptive réalisée auprès des médecins généralistes de Midi-Pyrénées.
- Bérénice Démailly. Étude du besoin de formation des médecins généralistes français àla gestion del’arrêt cardiaque. Médecine humaine et pathologie. 2018.
- Cwicklinski E. Gestion d’un arrêt cardiaque au cabinet médical: évaluation des connaissances et de la formation des médecins généralistes du département de la Vendée.The Med Nantes. 2012; 7: 77.
- Carole Gallois, Sandra Manesse, Nathaliedi Carmine, et al. Évaluation des connaissances de la prise en charge de l’arrêt cardiorespiratoire intrahospitalier : enquête de 365soignants. Anesthésie & Réanimation. 2015; 1: 312.
- Colquhoun MC. Defibrillation by general practitioners. Resuscitation. 2002 ; 52 : 143-148.
- Roger C, Lefrant JY, Bousquet PJ, et al. Formation des médecins généralistes aux gestes de réanimation d’urgence: Etude auprès des médecins généralistes de 4 départements du Sud de la France. La Presse Médicale. Tome 37, n°5. 2008.
- Shao H, Li CS. Epinephrine in Out-of-hospital Cardiac Arrest: Helpful or Harmful?. Chinese Medical Journal. 2017; 130: 2112-2116.