Efficacy of Triple Combination Antihypertensive Therapy in Hypertensive Patients with Pre-Diabetes
Author'(s): Nagay AV*, Khamidullaeva GA and Srojidiniva NZ
The Republican Specialized Center of Cardiology, Uzbekistan, Tashkent.
*Correspondence:
Aleksandr Nagay, Department of Arterial Hypertension and Molecular Genetics Research, Republican Specialized Center of Cardiology, 100052, Tashkent Uzbekistan, Tel: +998903503409; E-mail: alexsan1984@mail.ru.
Received: 02 May 2017; Accepted: 24 May 2017
Citation: Nagay AV, Khamidullaeva GA, Srojidiniva NZ. Efficacy of Triple Combination Antihypertensive Therapy in Hypertensive Patients with Pre-Diabetes . Diabetes Complications. 2017; 1-4.
Abstract
Aim of the study: evaluation of antihypertensive, organprotective efficacy and influence on metabolic disorders of triple combination antihypertensive therapy with valsartan, indapamide and amlodipine in hypertensive patients with pre-diabetes, who are resistant to bi-combination therapy.
Material and Methods: The study included 66 men with hypertension in average age of 56.06 ± 7.86 years, diagnosed abdominal obesity (waist circumference 103.11 ± 6.4 cm and body mass index 34.54 ± 3.83 kg/m²) and metabolic disorders, which were resistant to bi-combination antihypertensive therapy. The hypertensive patients with associated clinic conditions didn’t include to the study. Target organ damage (TOD) was diagnosed by Echocardiography and Ultrasound of brachiocephalic arteries. Microalbuminuria was determined on daily urine and glomerular filtration rate was calculated using EPI formulae. Lipids and fasten glucose levels, serum creatinine and uric acid were measurement by biochemical methods. All measurements were before and during 6 monthly therapies with valsartan (Nortivan, “Gedeon Richter”, Hungary), indapamide (Indap, PRO.MED. CS Praha, Czech Republic) and amlodipine (Normodipine, “Gedeon Richter”, Hungary) in average daily doses 135.65 ± 37.63 / 2.52 ± 1.4 / 7.5 ± 2.6 mg respectively.
Results: According to AH degree and founded risk factors and TOD, hypertensive patients with pre-diabetes were characterized as with high cardiovascular risk. Triple combination therapy showed high antihypertensive efficacy, achieving goal blood pressure level on 94% patients with decreased systolic BP on -22.26 ± 5.84% and diastolic BP on -21.1 ± 5.85%, significantly decreased of pulse BP. Heart rate beat didn’t change. Valsartan, indapamide and amlodipine combination characterized with significantly high cardioprotective, renoprotective efficacies and metabolic neutrality. Additional non-pharmacological interference, contributed to decrease of epicardial fat thickness and waist circumference, and positive influence to dyslipidemia.
Conclusion: During 6-monthly triple combination antihypertensive therapy with valsartan, indapamide and amlodipine 94% of hypertensive patients with pre-diabetes, who were resistant to bi-combination therapy achieved goal BP level with significantly target organ protection and positive influence to metabolic disorders.
Keywords
Introduction
The main components of a metabolic syndrome or pre-Diabetum are the arterial hypertonia (AH) and obesity, these components lead to development of an atherosclerosis, remodeling of heart and vessels. It is known that the clinical picture of a hypertonia at persons with an obesity and normal body weight can differ. The reason of hypertonia and an obesity development are the hyper activation of renin - an angiotensin - aldosteron systems (RAAS). Besides, it is established that fatty tissue is the major endocrine organ which produces more than 40 types of enzymes [1].
Patients with hypertonic and obesity treat group of very high cardiovascular risk (CVD risk), they often tap resistance to anti- hypertensive therapy. Choosing anti-hypertensive drugs from the main group, the emphasis is placed on metabolic neutrality concerning lipid and carbohydrate exchanges.
According to references of ESH/ESC - one of rational approaches are combinations of drugs as: blockers of RAAS/diuretics and blockers of RAAS/antagonists of calcium. These combinations showed high anti-hypertensive and organ protective efficiency [2-4]. However researches show that 1/3 patients with hypertonia of high risk need the prescription of three drugs [5]. So, we tried to study efficiency of three-component anti-hypertensive therapy (Valsartan, indapamide and amlodipine) at patients with hypertonia, with symptoms of pre-diabetes (AH, obesity, dislipidemiya) whom two-component therapy didn’t help.
Material and Methods
Study subject
The hypertensive patients with associated clinic conditions didn’t include to the study. The study included 66 men with hypertension in average age of 56.06 ± 7.86 years, diagnosed abdominal obesity (waist circumference 103.11 ± 6.4 cm and body mass index 34.54 ± 3.83 kg/m2) and metabolic disorders, which were resistant to bi- combination antihypertensive therapy (<140/90 mm. Hg).
Exclusion criteria
Exclusion criteria were, clinical evidence for cerebrovascular or coronary heart diseases, cardiac arrhythmia, heart failure, diabetes type II. To exclude the effects of estrogenic modulations of endothelium function, women were not enrolled.
Blood pressure monitoring
Office measurement of the ABP was taken at a stage before prescribe of a triad combination of therapy (before treatment), in 2 weeks, 1 month, the 3-and 6 months of a combination therapy.
Echocardiography and Ultrasound measurements
Target organ damage (TOD) was diagnosed by Echocardiography and Ultrasound of brachiocephalic arteries. Central hemodynamic parameters and left ventricular mass were estimated using M-mode echocardiography [6]. Left ventricular mass was indexed to body surface area (g/m2) to calculate LVM indexand left ventricular hypertrophy was defined as an LVM index of ≥125 g/m2.
Definition of microalbuminuria
Microalbuminuria was determined on daily urine and glomerular filtration rate was calculated using EPI formulae.
Metabolic disorder
Lipids and fasten glucose levels, serum creatinine and uric acid were measurement by biochemical methods. Biochemical researches were conducted before treatment and while 6 month combination therapies.
Anti-hypertensive therapy
All measurements were before and during 6 monthly therapies with valsartan (Nortivan, “Gedeon Richter”, Hungary), indapamide (Indap, PRO.MED.CS Praha, Czech Republic) and amlodipine (Normodipine, “Gedeon Richter”, Hungary) in average daily doses 135.65 ± 37.63 / 2.52 ± 1.4 / 7.5 ± 2.6 mg respectively. All patients were given dietary recommendations - to exclude consumption of animal fats and products with the raised cholesterin, decrease of consumption of salt till 5 grams per day, with including of 4-5 portions of vegetables and fruit per day. Also pedestrian walking within 30-45 minutes was recommended. Hypo glycemic drugs weren't prescribed. Stratification of cordial complications risk was carried out on SCORE scale.
Statistical analysis
The significance level for all the analyses was set at p<0.05. Statistical analyses were performed using Microsoft Office Excel 2007 and Statistica v6.0 (StatSoft, USA) software.
Protection of subjects
The medical information gathered during the study was treated confidentially except as may be required by the law. All patients gave informed consent, and the Ethics Committee of the Republican Specialized Center of Cardiology approved the study.
Results
Despite earlier carried out anti-hypertensive therapy, all patients didn't reach the target BP level before including in research. AH 1-st degree is taped at 30 patients (45,4%), 2nd degree at 27 (41%), and the 3rd degree at 9 patients (13,6%). Patients were characterized by existence of a target lesion organ and the expressed metabolic disturbances. According to ECG, LVH is taped at 54 patients (81,8%), diastolic dysfunction LV is diagnosed for 55 patients (83,3%), epicardial fat ≥3 mm thick is taped at 38 patients (57,6%). At 66,7% of patients there was thickening of the IMT complex of the general carotid more than 0,9 mm, the microalbuminuria in daily urine (30-300 mg / 24Ñ?) is taped at 14 patients (21,2%), less than 60 ml/min. / 1,73м2 defined depression of settlement GFR at 24 patients (36,4%).
All patients were characterized by existence of this or that type of a dislipidemiya. 78,8% and 74,2% of patients had rising of the general cholesterin (Total cholesterol) and a cholesterin of lipoproteins of low density (LDL cholesterol). At 66,6% of patients it is taped hyper-triglitseridemiya (TG), at 33,3% of patients had cholesterin of lipoproteins of high density (HDL cholesterol); 40 mg/dl. 32 patients (48,5%) had disturbance of glucose tolerance. The taped changes from organs of targets and disturbance of a lipid and carbohydrate metabolism characterized existence of high risk of CVD of patients with pre-Diabetum.
During 6 month three-component therapies there were reliable depressions of SBP, DBP, pulse BP and an average settlement value of BP (Table 1); at the same time heart rate didn't change. Extent of depression of SBP made -22, 26 ± 5, 84%, DBP of -21,1 ± 5,85%. The target BP level is reached at 62 patients (94%), at the same time at four patients who didn't reach the target BP level, degree of AH decreased from 3 to the 1st degree. Rising of pulse BP>60 mm Hg is regarded as a marker of a lesion of vessels, rigidity of arteries. At the expressed depression of SBP and DBP against the background of a combination therapy, depression of pulse BP is taped.
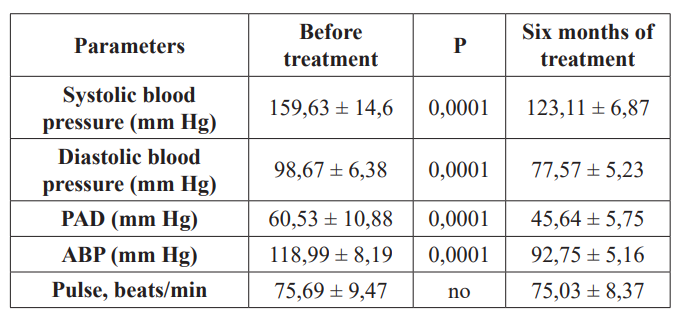
Table 1: Change of hemodynamic indicators against the background of 6-month therapy with valsartan, indapamid and amlodipine. *PAD- pulse blood pressure, ABP- average blood pressure.
The therapy of Valsartan/Indapamid/Amlodipin applied by us gave positive changes. Such approach promoted the return retrogress of LVH, decrease of thickness of IMT of the general carotid, improvement of diastolic function LV at hypertensive patients with an obesity (Table. 2).

Table 2: Markers dynamic of organs targets lesion against the background of 6 monthly therapy with valsartan, indapamid and amlodipine. *IVRT -Isovolumic relaxation time, IMT- Intima-media thickness, GFR- Glomerular filtration rate.
At the same time the number of patients without LVH was enlarged from 18,2% to 43,6%, at depression of LVM by 13%. Complex non-drug and drug treatment of patients with a hypertonia and obesity led to depression from and thickness of epicardial fat for 12%. Before therapy 24 (36, 4%) patients had the chronic illness of kidneys of IIIA of a stage. To the observation extremity only 10 patients (15%) had stage chronic illness of kidneys IIIA, at other 14 patients illness passed into the II stage that demonstrates improvement of a renal blood flow and protection of kidneys. In dynamics against the background of therapy of 7 sick microalbuminuria turned into norm.
As it was noted, sick AH with pre-Diabetum were characterized by imbalance of lipid and carbohydrate exchanges. Against the background of therapy of a lipid range of a blood it was characterized by a tendency to depression of the LDL level and rising of the HDL level and depression of aterogennost index (Table 3).
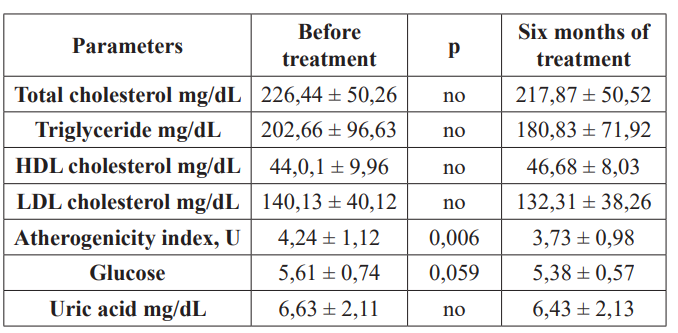
Table 3: Indicators dynamics of lipid, carbohydrate and purine exchanges against the background of 6 monthly therapy with valsartan, indapamid and amlodipin. * HDL - high density lipoprotein, LDL - low density lipoprotein.
There was tendency of depression of glucose level and decrease of number of patients with the broken tolerance to glucose from 48,5% to 28,8%. Level of uric acid remained invariable.
Discussion
In the last decades the wide circulation of obesity, imbalance of tolerance to glucose among patients with a hypertonia becomes perceptible. In our research there were 126 patients with hypertonia. At 26, 2% patients the increased body weight (n=33), at 65, 9% of sick (n=83) an obesity, at 7,9% of sick (n=10) – normal body weight is taped. 83 patients with an obesity of 66 patients were included in this research; other 17 patients had associated clinical states, including a diabetes 2 type. Difficult pathogenesis of AH in combination with an obesity explains need of a combination therapy. The most frequent combinations of two component therapies were - a blocker of RAAS/diuretics (58%), a blocker RAAS/betas-adreno blockers (26%), blockers of RAAS/ antagonists of calcium (16%). Thus, all patients before including in a research received rational combinations in a percentage ratio of RAAS/ ACE inhibitors of 40% of patients and the angiotenzive receptors blockers (ARB) of 60% of patients.
According to references on a hypertonia, triad therapy includes RAAS/blocker the diuretic/antagonist of calcium. As a result the patient refractory to double therapy, we prescribed valsartan/ indapamid/amlodipin. The patient accepting bisopropol before including in a research, drug was cancelled, reducing a dosage within 1 week.
At obesity fatty tissue becomes an additional important source of ATII synthesis Researchers showed that the ARB gives the most total block of RAAS [7]. Addition to ARB of a diuretic is justified from the pathogenetic point of view, especially, when at RAAS hyper activation, there is a delay of liquid and the volume of the circulating blood is enlarged. The vasoconstriction caused by hyper activation of RAAS leads to change of vessels, a prematurity of an atherosclerosis and aging of vessels. In this aspect intensifying of ARB combination + the diuretic + the antagonist of calcium interferes aging [8]. Besides, valsartan, indapamid and amlodipin proved high efficiency in many researches [9]. Thus, the combination of valsartan/indapamid/amlodipin is one of the possible rational combinations for treatment at obesity.
Results of our research showed high anti-hypertensive efficiency of a triad combination of drugs at sick AH with an obesity and metabolic imbalance, with achievement of the target BP level at 94% of patients. Metabolic neutrality of a triad combination gave positive changes. Tolerance of drugs was good. Side effects of drugs aren't revealed.
Conclusion
Hypertensive patients with pre-Diabetum for depression of BP and CVD need the combination therapy. The combination from three drugs – Valsartan/indapamid/amlodipin is recommended at not efficiency of a double combination therapy. Long observation of sick AH with pre-Diabetum against the background of therapy of Valsartan/indapamid/amlodipin showed high efficiency in 94%. At the same time there was observed good tolerance of drugs within 6 months. Such approach especially is suitable for treatment of sick AH having obesity.
Acknowledgments
We wish to thank the director, physicians, and nurses from the Republican specialized center of cardiology hospitals for their assistance in blood collection.
Financial and Competing Interest Disclosure
This work was supported by a Grant ADCC-15.13.1 from the Department of Health, Science and Technological Development of the Republic of Uzbekistan. The authors have no other relevant affiliations or financial involvement in any organization or no financial interest in or financial conflict with the subject matter or materials discussed in the manuscript.
References
- ESC Guidelines on diabetes, pre-diabetes and cardiovascular diseases developed in collaboration with the EASD (2013).
- ADVANCE Collaborative Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus. Lancet 2007; 370: 829-840.
- Dalhof B, Sever PS, Poulter NR, et Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindoprilas required vs. atenolol adding bendroflumethiazide as required in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA) a multicentre randomised controlled trial. Lancet 2005; 366: 895-906.
- Dahlof B, Devereux RB, Kjeldsen SE, et al. LIFE Study Cardiovascular morbidity and mortality in the Losartan Intervention for Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359: 995-1003.
- Bramlage P, Bohm M, Volpe M, et al. A global perspective on blood pressure treatment and control in a referred cohort of hypertensive J Clin Hypertens. 2010; 12: 666-677.
- ESH/ESC Guidelines Committee. 2013 Guidelines for the management of arterial hypertension. Guidelines Committee. Journal of Hypertension 2013; 31: 1281-1357.
- Aldo S. Villeco, Cinzia Cocci, Maurizio Di Emidio. Blood pressure control and weight loss in overweight or obese patients with previously treated or untreated mild to moderate hypertension given valsartan: an open-label study comparing pretreatment and treatment Current Therapeutic Research 2004; 65: 172-183.
- Matsui Y, Eguchi K, O’Rourke MF, et al. Differential effects between a calcium channel blocker and a diuretic when used in combination with angiotensin II receptor blocker on central aortic pressure in hypertensive patients. Hypertension 2009; 54: 716-723.
- Mancia G, Zanchetti A. Choice of antihypertensive drugs in the European Society of Hypertension-European Society of Cardiology guidelines: specific indications rather than ranking for general usage. J Hypertens 2008; 26: 164-168.