Epidemiological Aspects of Acute Coronary Syndromes in Saint-Louis, Senegal
Author'(s): Diop K.R1*, Ndao I2, Niasse A3, Beye S.M2, Mingou J.S1 , Diouf Y1, Ndiaye P.G1, Diop C.M.B1, Samb C.A.B3, Diouf M.T3, Aw F1, Sarr S.A1, Bodian M1, Ndiaye M.B1, Ad Kane2, Diao M1 and Kane A3
1Cardiology Department, CHU Aristide Le Dantec, Dakar, Senegal.
2Cardiology Department, Saint Louis Regional Hospital, Saint Louis, Senegal.
3Cardiology Department, Dalal Jamm Hospital, Dakar, Senegal.
*Correspondence:
K.R. Diop, Cardiology Department, CHU Aristide Le Dantec, Dakar, Senegal.
Received: 29 Oct 2022; Accepted: 02 Dec 2022; Published: 07 Dec 2022
Citation: Diop KR, Ndao I, Niasse A, et al. Epidemiological Aspects of Acute Coronary Syndromes in Saint-Louis, Senegal. Cardiol Vasc Res. 2022; 6(5): 1-6.
Abstract
Introduction: The prevalence of cardiovascular diseases has been rapidly increasing in developing countries, leading to an increasing incidence of acute coronary syndrome which is becoming a major health concern. Few studies have been conducted in hospital settings, which has led us to conduct this cross-sectional, descriptive study in Saint Louis in the north of Senegal, (250 km away from the capital) whose objective is to describe the epidemiological aspects of acute coronary syndrome (ACS) in hospital settings.
Methodology: This is a cross-sectional descriptive and retrospective study lasting two years from January 1, 2018 to 31 December 2019 which included all patients hospitalized in the cardiology department of the regional hospital of salary for an ACS.
Results: Out of 475 patients admitted to the department of cardiology, 47 presented with acute coronary syndrome which is a prevalence of 9.89%. The mean age was 63+/-13.14 years. There was a male predominance with a sex ratio of 1.5. The meantime between the beginnings of symptoms to hospitalization was 50 hours. The most frequent clinical presentation was acute coronary syndrome with ST segment elevation (STEMI: ST-segment Elevation Myocardial Infarction) in 39 patients. Hypertension was the most common cardiovascular risk factor in 23 patients and chest pain was the most common symptoms 72.3%. In STEMI patients, the ECG abnormalities were mainly in the anterior region and in NSTEMI (Non-ST-segment Elevation Myocardial Infarction) patients the ECG abnormalities were mainly in the inferior region. On echocardiography, 64% of patients had an altered left ventricular ejection function in STEMI patients whereas in NSTEMI patients, the left ventricular ejection function was preserved in 71% of cases. STEMI patients received within the first 12 hours represented 66% of our population of which 84% benefited from thrombolysis with streptokinase with a success rate of 52%. The mean time to thrombolysis was six hours. Six patients or 12.76% were sent for coronarography. The most common complication was cardiovascular collapse (11%), 15% of patients died.
Conclusion: The prevalence of acute coronary syndrome is increasing in West Africa with a predominance of ST segment elevation acute coronary syndromes. The main issues encountered were long leading times between onset of symptoms and hospital admission along with limited availability of medical facilities.
Keywords
Introduction
Over the course of the past two decades, the worldwide disease burden has shifted from mainly communicable, maternal and perinatal diseases, to non-communicable diseases [1].
Cardiovascular disease has become the leading cause of death worldwide related to non-communicable diseases with over 50% of deaths worldwide being attributed to it. The World Health Organization estimates that 17.6 million people worldwide died of cardiovascular diseases in 2012, representing 31.43% off all deaths worldwide, ischemic cardiomyopathies were responsible for 7.4 million deaths or 13.2% total. The burden of cardiovascular diseases weighs heavily on low- and middle-income countries, where 80% of these deaths occurred [1]. Their prevalence has been increasing in sub-Saharan Africa due to changing lifestyles, increasing prevalence of cardiovascular risk factors, increasing access to healthcare and an aging population [2-4]. In Senegal, the little data available regarding the hospital prevalence of acute coronary syndromes found the low prevalence of 4.05%. In Saint Louis of Senegal, there is little data available on acute coronary syndromes. This study is trying to fill the gap in knowledge by studying and analyzing acute coronary syndrome cases hospitalized in the cardiology department of the regional hospital of Saint Louis.
The main goal of this study is to record the epidemiological, clinical, paraclinical, therapeutic, and evolutive aspects of acute coronary syndromes.
Methods
This study was conducted in the department of cardiology of the regional Hospital of St. Louis (Senegal). This is an observational retrospective and cross-sectional study over 24 months from January 1, 2018 to December 31, 2019.
All patients admitted in the cardiology department for acute coronary syndrome, without distinction of sex, age, and nationality were included. Acute coronary syndromes were defined by: Clinical criteria, such as typical or atypical chest pain lasting for over 20 minutes Electrocardiography criteria, such as persistent ST segment elevation at point J and at least two contiguous or adjacent leads superior or equal to 2 mm (over 2.5 mm in men before 40 and over 1.5 mm in women in V2-V3.) or superior or equal to 1 mm in the other leads, recent appearance of a pathological Q wave or complete left bundle branch block or non-persistent ST elevation, or ST depression of over 1 mm horizontal or descending at point J, or a negative T wave in at least two continuous or adjacent leads. Biological criteria: an elevation of troponin over the 99th percentile of the upper limit of the reference range All patients who presented with stable angina were excluded
Studied Parameters
Sociodemographic data such as age and sex Cardiovascular risk factors: hypertension, which was defined as a systolic blood pressure superior or equal to 140 mmHg and or diastolic pressure superior or equal to 90 mmHg; diabetes, defined as a chronic disease characterized by the presence of excess sugar in the blood(hyperglycemia) the diagnosis is positive if the fasting glycemia is superior or equal to 1.26 g/L or 7 mmol/L for two consecutive tests; tobacco use, whether active, past (over 3 years before) or passive. Active is defined as smoking tobacco voluntarily; passive is involuntary inhalation of smoke from one or multiple smokers. Dyslipidemia defined as a total hypercholesterolemia, a HDL hypocholesterolemia, LDL hypercholesterolemia, or hypertriglyceridemia; obesity defined as a BMI over 30 kg/m2; abdominal obesity, which is a waist over 102 cm in men and over 88 cm in women. A personal or family history of cardiovascular disease.
Physical exam data: typical, or atypical resting angina, dyspnea, heart failure symptoms, pulmonary condensation syndrome, hemodynamic instability, murmurs, arrhythmias, timeframe from onset of symptoms and hospital admission.
EKG-data: acute coronary syndrome topography, rhythm and conduction abnormalities (atrial junctional and ventricular)
Cardiac Doppler ultrasound data: abnormal segmental kinetics (hypokinesia, akinesia, dyskinesia) and their topography. Left ventricular ejection fraction, measured using Simpson Biplan method. It was either preserved (over 50%) moderately reduced (between 30 and 50%) or severely reduced (under 30%). Complications: pericardial effusion, thrombus, left ventricular aneurysm, wall rupture…
Thrombolysis in STEMI patients: timeframe for thrombolysis and results. The criteria for success were clinical (decrease or disappearance of chest pain), electrical (ST elevation decreased by over 50%), reperfusion conductive injury (premature ventricular beats, ventricular tachycardia, accelerated idioventricular rhythm). It was considered unsuccessful if no criteria of success were found 45 minutes after thrombolysis.
Coronarography data: significant lesions (reduction over 50% of the artery’s diameter)
The data was typed in to the Excel software 2010 version and the analysis was done with the SPSS software 23rd version. This descriptive study was realized with the computation of frequencies and proportions for qualitative variables and computation of means for quantitative variables.
Results
Over the course of the study, 475 patients were hospitalized in the cardiology department of the regional hospital of St. Louis, among them were 47 acute coronary syndrome cases which is a hospital prevalence of 9.89%. There was a male predominance with 28 men (59.6%) to 19 women (40.4%) or a male to female sex ratio of 1.5. The mean age of the patient was 63 years (+/-13.14 years) old with ages ranging from 38 to 93 years. The mean time between symptom onset and hospital arrival was 50 hours with times ranging from one hour to 720 hours.
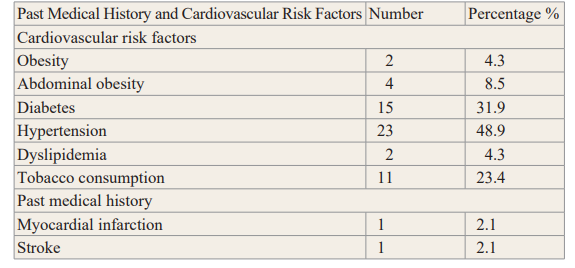
In our study 53% (n=25) of our total population and 66% of STEMI patients were admitted within the first 12 hours. 39 patients (83%) were admitted for acute coronary syndrome with persistent ST segment elevation or STEMI and eight patients (17%) for acute coronary syndrome without persistent ST segment elevation or NSTEMI. Hypertension was the most common cardiovascular risk factor and was present in 23 patients (48.9%) followed by diabetes in 15 patients (31.9%) and active tobacco use in 11 patients (23.4%). Six patients (12.8%) had no known cardiovascular risk factors. The table below shows the distribution of past medical history and cardiovascular risk factors
Table 1: Distribution of past medical history and cardiovascular risk factors.
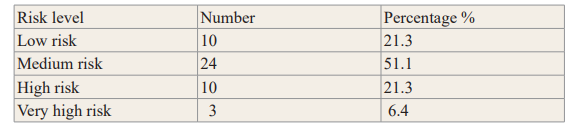
Moderate cardiovascular risk was found in 24 patients, low risk was found in 10 patients, high risk was found in 10 patients, and three patients have very high cardiovascular risk. The table below shows the distribution of patients according to their cardiovascular risk factors.
Table 2: Distribution of patients according to their level cardiovascular risk factors N=47.
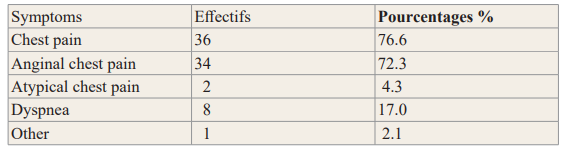
Chest pain what is the most common symptom and was present in 36 patients. The chest pain was anginal 34 patients and atypical in 2 patients. The table below shows the distribution of patients according to their presenting symptoms at admission
Table 3: Distribution of patients according to their presenting symptoms at admission (n=47)
Tachycardia was present in 39 patients and hypertension in six patients.
Pulmonary condensation syndrome was found in five patients, left heart failure in five patients, diabetic ketoacidosis in four patients and acute pulmonary edema in four patients. Physical examination was normal in 20 patients. Five patients presented with left heart failure (Killip II), two patients presented with cardiogenic shock (Killip IV), and for patients with acute pulmonary edema (Killip III). On the EKG, the STEMI lesions were located in 64% of cases in the anterior territory, in 28% of cases in the inferior territory, in 5% of cases in the circumferential territory, and 3% of cases in the lateral territory I need 3% of cases in the apical lateral territory.
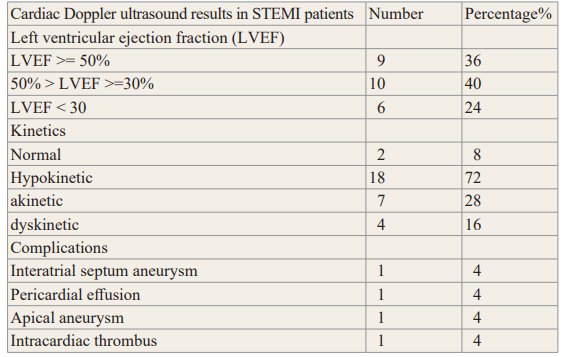
In NSTEMI patients, the ST segment depressions were located in 38% of cases in the inferior territory, and 13% of cases in the anterior territory 13% of cases in the lateral territory, there was also an inversion of the T-wave in septo-apico-lateral in 13% of cases and then lateral-apical in 13% of the patients. Nine (09) patients presented with conductive abnormalities: six (06) AV blocks of which four (04) were first degree and two were second degree and two right bundle branch blocks, and one left bundle branch block. Three patients had premature ventricular beats, two of them being NSTEMI patients. 32 patients underwent cardiac ultrasonography of which 25 were STEMI patients and seven were NSTEMI patients. For STEMI patients, left ventricular ejection fraction was preserved in 36% of patients. Ten (10) patients had moderately reduced ejection fraction and seven (07) patient had severely reduced ejection fraction.
Segmental kinetic troubles of the left ventricle were noted with 18 patients having hypokinesia, 7 having akinesia and 4 with dyskinesia. Intracardiac thrombus, pericardial effusion, and apical aneurysm were each found in one patient. The table below shows cardiac Doppler ultrasound results in STEMI patients.
Table 4: Cardiac Doppler ultrasound results in STEMI patients (n=25).
In NSTEMI patients the left ventricular ejection fraction was preserved and 71% of patients (N=5). One patient had moderate left ventricular dysfunction and severe dysfunction was found in another patient. Segmental kinetic troubles of the left ventricle were found such as hypokinesia in two patients and akinesia in one patient.
Among STEMI patients, 25 of them (84%) received thrombolysis with a success rate of 52% and streptokinase was the only molecule used. The meantime between symptom onset and thrombolysis was six (06) hours with tines ranging from one (01) hour and 45 minutes to 11 hours.
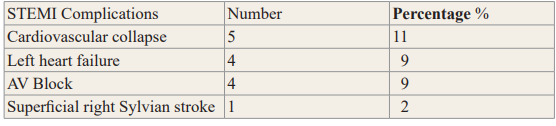
The most common complication was cardiovascular collapse in five (05) patients followed by left heart failure in for patients, AV block in for patients and an ischemic stroke in one patient. The table below shows complications.
Table 5: Distribution of patients according to complications.
The mean length of hospital stay please 6.36 days with stays ranging from 1 to 14 days for the study population.
Coronarography was realized in six (06) patients (12.76%). There was a single trunk lesion in four (04) patients of which two were localized in the left anterior descending artery, one (01) in circumflex artery, and the other in the right coronary artery. One patient had lesion on all three trunks.
Seven patients passed away from cardiogenic shock of which one was a NSTEMI patient and 40 patients were dismissed with beta- blockers, double antiplatelet therapy, statins and an ACE inhibitor.
Discussion
Limits of the study
The main limit to the study was the retrospective and monocentric characteristic.
In our study, the hospital prevalence of acute coronary syndrome was 9.85%. These numbers are greater than the numbers found by Mboup in 2014 who found a prevalence of 4.05% [5]. In Abidjan N’Guetta found a prevalence of 13.5% in 2016 [6]. There has been an increase in prevalence of acute coronary syndromes in Africa, which was 3.27 in 1991 in the CORONAFRIC study [7]. In Europe, there has been a notable reduction in acute coronary syndromes in the past 10 years [8]. The increased prevalence in Africa could be due to lifestyle modifications, and better diagnostic means [7].
In this study, there is a male predominance (59.6%) with a sex ratio of 1.5. This male predominance was correlated to that observed in coronary disease, which varies between 65 and 80% in Africa and in the West [9,10]. The difference between genders could be explained by the protective effect of estrogens in women, which disappears after menopause. The mean age of patients was 62.93+/- 13 years old ranging from 38 to 90 years old with a predominance for patients aged over 60. This is not reflective of previous African series where acute coronary syndromes happened earlier with a mean age under 60 [5,6,11].
The elderly population in Saint Louis only represents 6% according to the National Agency of Statistics and Demographics [12], this high prevalence of acute coronary syndrome in elderly people can be explained by multiple cardiovascular risk factors and comorbidities in this age group.
The mean time between symptom onset and hospital admission was 50 hours with times ranging from one (01) hour to 720 hours. This reflects the general trend in sub-Saharan Africa. The delay in contacting a medical professional and achieving efficient hospital transport creates a significant hinderance to early hospital admission in sub-Saharan Africa, which could take 6 to 10 days [6,13]. In Africa, transporting patients to the hospital often uses urban and rural public transport if available at the time or private cars and paramedical offices are particularly solicited [5,14]. This is explained by low awareness of African population on cardiovascular diseases. In addition, on the need to use a paramedical office for chest pain However, with the recent rise of cardiology in big African cities, the period between symptom onset and hospital admission, has been significantly decreasing in recent years. A recent study has shown the mean timeframe between symptom onset and first medical contact is 12.7 hours in some countries [15]. In our study, 66% of patients were admitted within the first 12 hours.
In this series, there is a higher prevalence of STEMIs at 83%. This is similar to the data of Mboup and N’Guetta who also found a higher STEMI prevalence [5,6]. 48.9 percent of our patients had hypertension. The INTERHEART study [3], which took place in 52 countries across the world shows that hypertension, is a more commonly associated risk factor for myocardial infarction in the African population than in the overall population. Diabetes prevalence in our study was 31.9% and 23.4% of our population consume tobacco. According to previous studies, tobacco consumption and diabetes are major risk factors for acute coronary syndromes [16].
In our study, hyperlipidemia had a prevalence of 4.3%. The link between high LDL cholesterol, low HDL cholesterol, and the risk of myocardial infarction is well-documented [3]. Within our population 43% presented with a normal physical exam.
In STEMI patients included in our study, the most common area that was affected in EKGs was the anterior region (64%), followed by the inferior region (28%) which correlates to Mboup’s data found, where there was a 61% prevalence of anterior and 33.9% of inferior territory abnormalities [5]. A Tunisian study found a predominance of the anterior region in 53% of cases [14].
In our study, 32 patients received an ultrasound of which 25 were STEMI patients and seven were NSTEMI patients. In STEMI patients, 92% of patients had altered segmental kinetics with a predominance for hypokinesia in 72% of patients, followed by akinesia in 28% of patients and dyskinesia in 16% of patients. The left ventricular ejection fraction was preserved in 36% of patients, moderately reduced and 40% of patients and severely reduced in 24% percent of patients. This is different from the results of Maurin and al who found the left ventricle ejection fraction was preserved in 17% of patients, moderately reduced in 14% of patients and severely in 4% of patients [17].
In NSTEMI patients the majority of the population had normal kinetics (62.5%), 37.5% had altered segmental kinetics of which 29% had hypokinesia and 14% had akinesia. The left ventricular ejection fraction was preserved in 71% of patients.
In our study, 66% of STEMI patients were admitted within the first 12 hours, of which 80.76% received thrombolysis and 52.38% of those were successful. All thrombolysis was done with streptokinase. The mean time frame during which process was achieved in six hours with times ranging from one (01) hour and 45 minutes to 11 hours. In the CORONAFRIC study, 34% of STEMI were thrombolysed with the mean time frame being 8.76 hours and 93.6% used streptokinase [18]. The high cost and low availability of other thrombolytic agents are the reason that streptokinase is the most used molecule in our geographic area.
In STEMI patients, the most frequent complication in our study was cardiovascular collapse (Killip IV) which occurred in 11% of the population. This rate was superior to that found in the register FAST-MI where a frequency of 4% was found. Left heart failure what is the second most common complication, and was found in 9% of the population. This prevalence is similar to that found by Mboup (10%) [5].
In NSTEMI patients, the only complication found was left heart failure in 25% of patients. The main length of hospital stay was 6.36 days with stays ranging from one to 14 days. Coronarography was performed on six patients or 15.38%. Due to the scarcity of interventional cardiology operating rooms in sub-Saharan Africa, the rate of patients receiving coronarography is very low compared to higher income countries. In St. Louis, no interventional cardiology operating room exists; therefore, all patients have to be transferred to the capital, which is a three hour or 250 km road trip. If primary angioplasty cannot be done within two hours of STEMI diagnosis, fibrinolytic treatment is recommended within the first 12 hours from symptom onset in patients without contraindications (Recommendation IA) [19,20]. This explains why none of the patients within the study were able to receive primary angioplasty. In addition to this geographic inaccessibility, was a financial one, the mean cost of coronarography is 500,000. FCFA (763euros) whereas the minimum salary is 48,000FCFA per month (73 euros per month). In this study, there was a hospital mortality rate of 15% which is similar to that found by Mboup (15.25%.), but inferior to that of Maurin et al. who found 20%.
References
- McAloon CJ, Boylan LM, Hamborg T, et al. The changing face of cardiovascular disease 2000-2012: An analysis of the world health organisation global health estimates data. Int J Cardiol. 2016; 224: 256-264.
- Mensah Ischaemic heart disease in Africa. Heart BMJ Publishing Group Ltd. 2008; 94: 836-843.
- Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control Lancet. 2004; 364: 937-952.
- Ntsekhe M, Damasceno A. Recent advances in the epidemiology, outcome, and prevention of myocardial infarction and stroke in sub-Saharan Africa. Heart. 2013; 99: 1230-1235.
- Mboup MC, Diao M, Dia K, et al. Les syndromes coronaires aigus à Dakar: aspects cliniques thérapeutiques et évolutifs. Pan Afr Med J. 2014; 19: 126.
- N’Guetta R, Yao H, Ekou A, et al. Prévalence et caractéristiques des syndromes coronariens aigus dans une population d’Afrique subsaharienne. Annales de Cardiologie et d’Angéiologie. Elsevier. 2016; 59-63.
- Ticolat P, Bertrand E, Longo-Mbenza, et al. Aspects épidémiologiques de la maladie coronaire chez le Noir Africain: à propos de 103 cas. Résultats de l’enquête multicentrique prospective CORONAFRIC 1. Cardiol trop. Marseille: Cardiologie tropicale. 1991; 17: 7-20.
- Danchin N, Puymirat E, Aissaoui N, et Épidémiologie des syndromes coronaires aigus en France et en Europe. Annales de cardiologie et d’angeiologie. Elsevier. 2010; S37-S41.
- Teo KK, Ounpuu S, Hawken S, et Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. The Lancet. 2006; 368: 647-658.
- Hanssen M, Cottin Y, Khalife K, et al. French Registry on Acute ST-elevation and non-ST-elevation Myocardial Infarction FAST-MI 2010. Heart. BMJ Publishing Group Ltd and British Cardiovascular Society. 2012; 98: 699-705.
- Bahiru E, Temu T, Gitura B, et al. Presentation, management and outcomes of acute coronary syndrome: a registry study from Kenyatta National Hospital in Nairobi, Kenya. Cardiovasc J Afr. 2018; 29: 225-230.
- Caractéristique démographique de la population de saint louis du Sénégal [Internet]. Disponible sur: Google https://www.sn.Caractéristiquedémographiquedelapopulationdesaintlouisdusénégal.consultéle15août2021à19h4513.
- Yameogo NV, Samadoulougou A, Millogo G, et al. Delays in the management of acute coronary syndromes with ST-ST segment elevation in Ouagadougou and factors associated with an extension of these delays: a cross-sectional study about 43 cases collected in the CHU-Yalgado Ouédraogo. The Pan African Medical Journal. 2012; 13: 90.
- Sami M, Hassen A, Ahmed S, et al. Prise en charge du syndrome coronarien aigu avec sus décalage du segment ST dans l’hôpital régional de Médenine. A propos de 150 cas. Cardiologie Tunisienne. 2017; 2: 25-32.
- Beza L, Leslie SL, Alemayehu B, et al. Acute coronary syndrome treatment delay in low to middle-income countries: A systematic review. Int J Cardiol Heart Vasc. 2021; 35:
- Pedrix C, Beaufils P. Complications de l’infarctus du myocarde. Evolution et pronostic. EncyclMédChir, Paris, Elsevier, Cardiologie. 1998; 11: 15.
- Maurin O, Massoure PL, de Regloix S, et Acute myocardial infarction in Djibouti: 2-year prospective study. Medecine et Sante Tropicales. 2012; 22: 297-301.
- Ba A. Epidémiologie de la coronaropathie en Afrique : étude CORONAFRIC-2. Congrès APPAC, 22 novembre 2017. Biarritz. [En ligne]. Disponible sur : https://www.google.com/search.EpidémiologiedelacoronaropathieenAfrique/.Consultéle11Août2021.
- Kakou-Guikahue M, N’Guetta R, Anzouan-Kacou JB, et al. Optimizing the management of acute coronary syndromes in sub-Saharan Africa: A statement from the AFRICARDIO 2015 Consensus Archives of Cardiovascular Diseases. 2016; 109: 376-383.
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39: 119-177.