Epidemiological, Clinical, Para-Clinical and Evolutionary Aspects of Diabetic Ketoacidosis At Abass Ndao Hospital
Author(s): Sow Djiby*, Diedhiou Demba, Dieng Mouhamed, Djiba Boundia, Ndour Michel Assane, Diallo Ibrahima Mané, Fall Ndiouga, Sall Ibrahima, Gadji Fatou Kiné, Sarr Anna, Ndour Mbaye Maimouna
Faculty of Medicine, Cheikh Anta Diop University/Internal Medicine Department, Abass Ndao Hospital, Dakar.
*Correspondence:
Dr. Djiby SOW, Maitre-Assistant, Clinique Médicale II, Centre Hospitalier Abass Ndao, Cheikh Anta DIOP University, Dakar, Tel: 00221 77 6402662.
Received: 11 Sep 2023 Accepted: 13 Oct 2023 Published: 20 Oct 2023
Citation: Sow Djiby, Diedhiou Demba, Dieng Mouhamed, et al. Epidemiological, Clinical, Para-Clinical and Evolutionary Aspects of Diabetic Ketoacidosis At Abass Ndao Hospital. Diabetes Complications. 2023; 7(1); 1-5.
Abstract
Introduction: Diabetes is a public health problem, exposing patients to serious complications including ketoacidosis. The aim of this study was to describe the epidemiological, therapeutic and evolutionary aspects of diabetic ketoacidosis at the Abass ndao hospital in Dakar.
Patients and Methods: This was a cross-sectional, descriptive study conducted from January 01, 2016 to December 31, 2016. It focused on diabetic patients hospitalized for diabetic ketoacidosis. A standard questionnaire was drawn up to serve as the basis for data collection.
Results: One hundred and forty-three (143) cases of ketoacidosis were reported, representing a frequency of 18.94%. The mean age of patients was 46.52 years, with extremes of 15 and 87 years. The age groups [41-50] and [61-70] were the most represented with 19.6%. The female gender was more represented with 79 women (55.2%) with a sex ratio (f/h) equal to 0.81 Housewives were the most represented with 26.57%. Patients were predominantly from the Dakar region, with 133 cases (93%). Type 2 diabetes was predominantly represented with 66.4%. Diabetes had been evolving for less than 5 years in 60% of patients. Hypertension was present in 56 of our patients (39.16%). The average hospital stay was 18.46 days. Twenty-four patients (9.79%) were seen after 15 days. The most frequent reasons for hospitalization were polyuria-polydipsia with 54 cases or 37.76%, followed by dyspnea with 40 cases or 27.97%. Diabetic precoma was noted in 27 cases (9%). Twenty patients presented with fever (13.98%). An infectious factor of diabetic imbalance was noted in 73 patients (51.04%), and 34 patients (46.57%) had a respiratory infection. Diet deviations were noted in 20 patients (13.98%). MI was noted in 7 patients (46.66%). Hyperleukocytosis was found in 64 patients (44.75%), and CRP was elevated in 100 patients (74.62%). Mean capillary blood glucose was 3.3942 g/l. Ketonuria was greater than or equal to 2x in 143 patients (100%). Renal function was impaired in 57.34% of cases. Mean kalemia was 4.33meq/l, with extremes of 0.5 and 7meq/l, and hypokalemia was present in 30.06% of cases. Hyponatremia was found in 22.81%. Cardiac electrical disturbances were noted in 43 patients, or 30.06% of cases, revealing ischemic heart disease in 7 patients. The average length of stay was 8.43 days, with extremes of 1 and 42 days. There were 30 deaths (20.97%).
Conclusion: Diabetic ketoacidosis is a serious complication. It requires appropriate management and therapeutic education of patients.
Keywords
Introduction
Diabetes is a public health problem. According to the International Diabetes Federation (IDF), an estimated 366.2 million people worldwide suffer from diabetes mellitus. Of these, 14.7 million live in Africa. IDF experts predict that 552 million adults will have diabetes by 2030.
It's a formidable metabolic disease because of its usually insidious course. This exposes patients to chronic degenerative complications, as well as acute metabolic complications requiring long and costly treatment. These acute complications deserve particular attention, including ketoacidosis. This results from absolute or relative insulin deficiency, with the immediate consequence of hyperglycemia and ketosis, responsible for hydroelectrolytic disorders. However, ketoacidosis remains a major clinical problem in our time. Indeed, its incidence continues to rise, affecting an ever wider range of populations. The mortality and morbidity associated with it remain significant. The general aim of this study is to describe the epidemiological, clinical, paraclinical and evolutionary aspects of diabetic ketoacidosis received in the emergency department of the Abass Ndao Hospital.
Materials and Methods
The study was carried out in the emergency department of the Abass Ndao Hospital in Dakar.
This was a descriptive cross-sectional study of diabetic subjects seen in emergency departments with signs of urinary tract infection. Our patients were recruited over a one-year period (January 01, 2016 to December 31, 2016). The study population consisted of known or unknown diabetic patients, regardless of type and origin, received at the Abass Ndao hospital emergency department. All diabetic patients admitted to the Abass Ndao hospital emergency department during the recruitment period for diabetic ketoacidosis were included in our study.
- Blood glucose > 2.5 g/L
- Positive ketonuria
With the presence of at least one of the following criteria:
- Hypokalemia on admission (< 5mmol/L)
- Systolic blood pressure < 90mmHg
- Heart rate > 100 or < 60 bpm
All diabetic patients without ketoacidosis and with incomplete records during the recruitment period were not included in our work.
Data Collection Procedure
Collection tools
A standard questionnaire was drawn up to serve as the basis for data collection for patients included in the study. It covered marital status, clinical and paraclinical manifestations, diabetes study and hospitalization outcome.
Sources of collettes
Data were collected from the records of patients fulfilling the inclusion criteria.
Study Variables
The data collected concerned:
- Socio-economic characteristics: age, gender, profession, place of origin
- Clinical characteristics - Study of diabetes mellitus: The study of diabetes focused on the type of diabetes, how long it had been present, how well it was balanced, and whether or not there were other cardiovascular risk factors (smoking, hypertension, dyslipidemia, age, alcoholism). Sedentary lifestyle was not
Patients were considered hypertensive if systolic blood pressure was greater than or equal to 140mmHg and/or diastolic blood pressure greater than or equal to 90mmHg, or if blood pressure figures were normal on antihypertensive treatment [7]. Diabetes typing, in the absence of immunology and C-peptide assay, was presumptive based on clinical and evolutionary arguments (patient's age, morphotype, time to onset of symptoms, family history and evolution under treatment).
History and vitals: BP, HR, RF, SaO2, temperature, diuresis, capillary glucose, glucosuria and ketonuria.
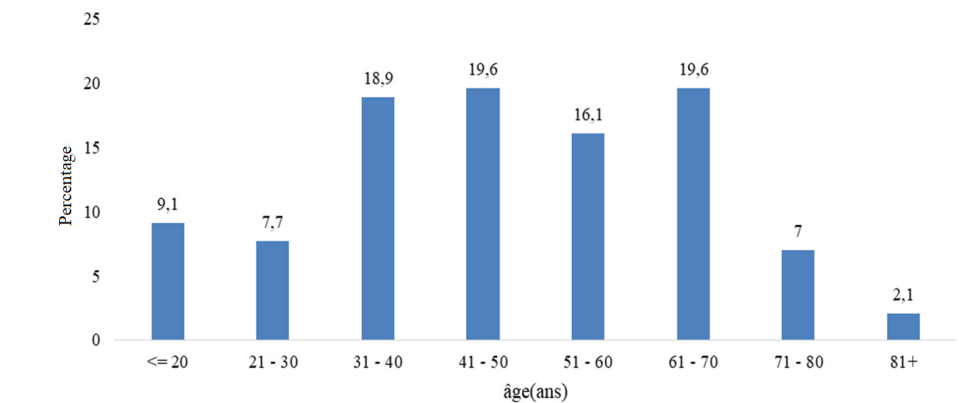
Figure 1: Patient distribution by age group.
Paraclinical characteristics
These included CBC, creatinine and uremia levels, CRP, HbA1c, fasting blood glucose, lipid profile, blood culture, thick blood drop, blood ionogram, ECBU, electrocardiogram (ECG), cardiac Doppler ultrasound, lower limb Doppler ultrasound, foot X-ray, chest X-ray, brain scan, etc.
- analysis of triggering factors: (therapeutic errors, infectious conditions, other...).
Evolutionary profile: Evolutionary characteristics (mean length of hospital stay, mortality, complications) were noted.
Data capture and analysis
Data were entered using Microsoft Office Excel and analyzed using epi info 2000 version 3.3.2. During analysis, we calculated frequencies and means with standard deviations.
Results
Socio-demographic characteristics
During the study period, 755 patients were hospitalized in the emergency department. Of these, 143 presented with diabetic ketoacidosis, a frequency of 18.94%. The average age of patients was 46.52 years, with extremes of 15 and 87 years. The age groups [92-101] and [43-46] were the most represented with 19.6%. Females were more represented, with 79 women (55.2%) for 64 men (44.8%), with a sex ratio (F/H) equal to 0.81. Housewives were the most represented with 26.57%, followed by shopkeepers with 22.37%. The majority of patients came from the Dakar region, with 133 cases (93%).
Clinical aspects
Type 2 diabetes was predominant in 95 cases (66.4%). The majority of our patients had had diabetes for less than 5 years, with 86 cases (60%), and hypertension was the main risk factor associated with diabetes, present in 56 cases (39.16%). A family history of diabetes was noted in 30 cases (20.97%), with an average hospital stay of 18.46 days, ranging from 1 to 540 days. 24 patients (9.79%) were seen after 15 days. The most frequent reasons for hospitalization were polyuria-polydipsia with 54 cases (37.76%), followed by dyspnea with 40 cases (27.97%). A diabetic pre-coma was noted in 27 cases (9%) and a coma in 22 cases (15.3%). The mean heart rate was 95.53 beats/min, with extremes of 51 and 178 beats/min. Fever was present in 20 patients (13.98%). An infectious imbalance factor was noted in 73 patients (51.04%). Diet deviations concerned 20 patients (13.98%). Of the 73 patients with an infectious pathology, 34 (46.57%) had a respiratory infection. MI was noted in 7 patients (46.66%). Stroke occurred in 4 cases. The cause could not be determined in 21 patients.
Anemia was found in 65 patients (45.45%). The mean white blood cell count was 22.21,000 G/L, with extremes ranging from 2.57,000 to 23.20,000 G/L. Hyperleukocytosis was found in 64 patients (44.75%), and CRP was elevated in 100 patients (74.62%). Mean capillary blood glucose was 3.3942 g/l.100 patients had glycosuria greater than or equal to 2x, i.e. 69.93%. All patients had ketonuria greater than or equal to 2x (100%). Renal function was impaired in 57.34%. Mean kalemia was 4.33meq/l, with extremes ranging from 0.5 to 7meq/l, and hypokalemia was present in 30.06% of cases. Hyponatremia was found in 22.81%. Electrical disturbances were noted in 43 patients, or 30.06% of cases, revealing ischemic heart disease in 7 patients.
Evolution
The average duration was 8.43 days, with extremes of 1 and 42 days. We observed 30 deaths (20.97%).
|
Reasons for hospitalization |
Workforce |
Percentage (%) |
|
Polyuria-polydipsia |
54 |
37.76 |
|
Kusmaul's dyspnea |
40 |
27.97 |
|
Asthenia |
8 |
5.59 |
|
Impaired general condition |
19 |
13.28 |
|
Fever |
20 |
13.98 |
|
Anorexia |
20 |
13.98 |
|
Headaches |
20 |
13.98 |
|
Urinary burning |
3 |
2.09 |
|
Cough |
5 |
3.49 |
|
Lower limb pain |
15 |
10.48 |
|
Motor deficit |
1 |
0.69 |
|
Polyphagia |
3 |
2.09 |
|
Lower limb wounds |
15 |
10.48 |
|
Cardiovascular collapse |
4 |
2.79 |
|
Convulsive seizures |
2 |
1.39 |
|
Gait disorder |
2 |
1.39 |
|
Palpitation |
1 |
0.69 |
|
Chest pain |
4 |
2.79 |
|
Big painful leg |
5 |
3.49 |
|
Lower back pain |
3 |
2.09 |
|
Dysuria |
2 |
1.39 |
|
Visual blur |
1 |
0.69 |
|
Cervical mass |
1 |
0.69 |
|
Bleeding |
1 |
0.69 |
|
Gastroesophageal reflux disease |
1 |
0.69 |
|
Syncope |
1 |
0.69 |
Table 1: Distribution of patients by reason for hospitalization.
|
Pathologies |
Workforce |
Percentage (%) |
|
Infectious |
73 |
51.04 |
|
Drug reactions |
20 |
13.98 |
|
Cardiovascular |
15 |
10.48 |
|
Endocrine |
1 |
0.69 |
|
Hematological |
1 |
0.60 |
|
Neurological |
4 |
2.79 |
|
Gastroenterology |
1 |
0.69 |
|
Neoplastic |
1 |
0.69 |
|
Idiopathic |
21 |
14.68 |
|
Urological |
6 |
4.19 |
|
Total |
143 |
100 |
Table 2: Distribution of imbalance factors.
|
Infectious diseases |
Workforce |
Percentage (%) |
|
Respiratory infections |
Respiratory infections |
34 |
|
Urogenital infections |
Urogenital infections |
15 |
|
Skin and soft tissue infections |
Skin and soft tissue infections |
12 |
|
Digestive tract infections |
Digestive tract infections |
4 |
|
Malaria |
Malaria |
2 |
|
Neurological infections |
Neurological infections |
2 |
|
Sepsis |
Sepsis |
1 |
|
ENT infection |
ENT infection |
1 |
|
Stomatological infection |
Stomatological infection |
1 |
|
Osteoarticular infection |
Osteoarticular infection |
1 |
|
Total |
Total |
73 |
Table 3: Distribution of infectious pathologies.
Discussion
Epidemiological data
Diabetic ketoacidosis was 18.94% in our study. In the study by Lokrou A in Abidjan, the prevalence of ketoacidosis was higher than ours (30.7%) [1]. Placide et al. in Lubumbashi found a prevalence of 37.2%, and it was the most frequent acute metabolic complication of diabetes in his study [2]. In a Yaoundé intensive care unit, Jemea B et al. found a very low frequency of 1.16% [3]. The same result was found in Tchaou, Benin (7.8%) [4]. Our prevalence may be explained by our proximity to the national reference center for diabetes management. In Touba, Ka O et al. found a prevalence of ketoacidosis much higher than ours (61.8%) among patients [5]. Its annual incidence in the United States of America (USA) is estimated at between 4.6 and 8 episodes/1000 diabetics, with a steady increase [7].
The mean age of patients was 46.52 years, with extremes of 15 and 87 years. In the study by Leye et al. in Senegal, the mean age of patients was 46.78 years, with extremes ranging from 17 to 84 years [6]. The most representative age group was made up of patients aged 45 to 59 (36.78%). This is close to our study. In the Sarra J study in Tunisia, the mean age was 38 +/- 18 years, which is lower than ours [8]. Placide K in his series found an average age of 44.8 years [2]. In the international literature, the mean age at onset of ketoacidosis varies from 31 to 45 years, depending on the series [9].
The female sex was more represented with 79 women (55.2%) for 64 men (44.8%) with a sex ratio (F/H) equal to 0.81. This result is close to that obtained by Lèye YM and Sarra J with a respective ratio of 0.44 and 0.94 in favor of women [6,8]. Contradictory results were also found by Placide K in Lubumbashi, with a sex ratio of 1.42 [2]. The majority of patients came from the DAKAR region, with 133 cases (93%). Similar results were found by Leye et al. [6]. The majority of his patients (92.16%) came from the suburbs of Dakar.
Clinical Data Hospitalization time
The average hospital stay was 18.46 days. 80 patients (55.94%) consulted us before 7 days. This means that we need to reinforce our patients' therapeutic education to consult immediately in the event of hyperglycemia. This is higher than that observed by Simon A and Elmehdawi in Libya, whose studies reported hospitalization times of 4.09 days and 2.7 days respectively [10,11].
Length of hospital stay
The average length of stay was 8.43 days, with extremes of 1 and 42 days. Sarra J's average length of hospital stay in the emergency department was 61+/- 42 hours [8]. In Placide K's study, the mean length of hospital stay was similar to ours, at 9.3 days [2].
Diabetes study
Type 2 diabetes was predominantly represented at 66.4%. This result corroborates those found by Lèye et al. 65.68% [6]. In Conakry, Baldé et al. found 95% type 2 diabetes [13]. The majority of our patients had diabetes evolving for less than 5 years, with 86 cases (60.0%). In Benin, Simon A found a similar age of diabetes to our study [10]. Contradictory results were found in Senegal by Leye et al. [6], where 61.76% of patients were known diabetics, with an average duration of progression of 10 years. Mean capillary blood glucose was 3.39 g/l. Leye Y in Senegal found a higher result than ours, with a mean blood glucose level of 4.10 g/l [6]. In the same study, the mean HbA1C level was 11.17%. This is close to our study.
Reasons for hospitalization
The most frequent reasons for hospitalization were the polyuria- polydipsia association with 37.76%, followed by dyspnea (27.97%). Placide et al. [2] reported dyspnea (80.4%), the polyuria- polydipsia syndrome (76.5%) and altered consciousness in 58.8% of cases. Leye et al. [6] found disorders of consciousness in 25.5% of patients.
Decompensation factors
Seventy-three (73) patients had an infectious pathology (51.04%). Of these, 34 patients (46.57%) had a respiratory infection. In Senegal, Wade K et al. found a predominance of infectious factors in 64% of cases [14]. This is lower than that observed by Sarra J. Indeed, in 32% of patients presenting with an infectious pathology, 14.5% had a respiratory infection [8]. Elsewhere, an infection was found in 66.67% of patients, with a predominance of urogenital infections (38.23%) and pneumopathy (29.42%) [6].
Skin infections were noted in 16.43% of patients. These skin infections dominate the infectious reasons for hospitalization in our diabetic patients, due to the existence of a diabetic foot unit in the national diabetes management center. In the study by Sow D et al., the prevalence of infections among diabetics was found to be 50% [18]. However, in their study, infections were dominated by skin and soft tissue infections (54.9%), urogenital infections (16.2%) and respiratory infections (14.4%) [18]. The cause could not be determined in 21 patients. The same findings were made inConakry 5% in his series [13]. Monabeka et al. in Congo reported 12.3% of undetermined cause.
Paraclinical data
More than the majority (57.34%) had impaired renal function. In Morocco, Noto-Kadou-Kaza et al. reported a 44% prevalence of AKI in patients admitted for DKA [16]. The mean kalemia was 4.33meq/l and hypokalemia was noted in 30.06%. In the Sarra J study in Tunisia, hypokalemia was present in 43% [8]. This is higher than ours. In Leye's series, the mean kalemia was close to our study (4.1 mmol/l and hypokalemia in 18.63%) [6].
Evolution
Mortality in our study was 20.97%; in Lubumbashi, the case- fatality rate was 27.5% [2]. In Kenya, the mortality rate was 33% AND 44% in Johannesburg [17]; for SARRA J, it was 2.1% [8].
References
- Lokrou A, Kouassi F. Assessment of 9 years of management of ketoacidosis in adult African diabetics in Côte dIvoire. Médecine des Maladies Métaboliques. 2014; 8: 330-334.
- Placide Kambola Kakoma, David Mulumba Kadiebwe, Axel Mbuyu Kayembe, et al. Diabetic ketoacidosis in adults at Sendwe Hospital in Lubumbashi about 51 cases. Pan African Medical 2014; 17: 324.
- Jemea B, Bengono BR, Gouag Ndongo AS, et Complications Aiguës Métaboliques du Diabète en Réanimation Epidémiologie Prise en Charge et Pronostic à Yaoundé. Health Sci Dis. 2021; 22: 42-46.
- Mobio MP, Nétro D, Olama MC, et al. Prognostic factors of metabolic complications of diabetes mellitus in an intensive care unit in Rev Afr Anesthésiol Med Urg. 2017; 22: 9-13.
- Ka O, Sow D, Yade B, et al. Profil des diabétiques hospitalisés au service de Médecine Interne de lhôpital Ndamatou de Touba Sénégal. MALI SANTE 2021; XI : 2.
- Leye A, Ndiaye N, Diack N, et Epidemiological and diagnostic aspects of diabetic ketoacidosis in hospitals in Dakar Analyse de 102 cas au CHU de Pikine RAFMI. Revue Africaine de Médecine Interne. 2016; 3: 8-11.
- Orban JC, Ichai Acute metabolic complications of diabetes. Resuscitation. 2008; 17: 761-767.
- Sarra Jouini, Asma Aloui, Olfa Slimani, et Epidemiological profiles of diabetic ketoacidosis in emergency departments. Pan Afr Med J. 2019; 33: 322.
- Rheeder P, Stolk RP, Grobbee DE, et Ethnic differences in C peptide levels and anti Gad antibodies in south African patients with Diabetic Ketoacidosis. QJ Med. 2001; 94: 39-43.
- Simon complications aiguës metaboliques du diabète sucre dans lunité de réanimation de lhôpital universitaire de parakou. European Scientific Journal. 2014; 10: 24.
- Elmehdawi RR, Elmagerhei Profile of diabetic ketoacidosis at a teaching hospital in Benghazi Libyan Arab Jamahiriya. East Mediterr Health J. 2010; 16: 292-299.
- Abdulrahman GO, Amphlett B, Okosieme OE, et Trends in hospital admissions with diabetic ketoacidosis in Wales 1999- 2010. Diabetes Res Clin Pract. 2013; 100: e7-10.
- BALDÉ NM, Barry AY, Diallo MM, et Ketoacidosis during diabetes mellitus in Conakry frequency and decompensation factors need for targeted education Annales de lUniversité de Ouagadougou. Série D. 2006; 4: 2006.
- Wade KA, Diallo A, Niang EHM, et Prise en charge de la cétoacidose diabétique dans le service de réanimation médicale de lhôpital principal de Dakar Sénégal. RAMUR Tome. 2011; 16: 2.
- Monabeka HG, Nicole Nsakala Ketoacidotic coma inaugurating diabetes in black adults. Santé. 2001; 11: 127.
- Béfa Noto kadou kaza . EYM Amekoudi GN Imangue Okouango AY Bikinga Wendkuuni AH Mahamat J Badibanga Tsikpamba CM Tsevi MG Benghanem B Ramdan Acute renal failure during diabetic ketoacidosis in the intensive care Health Sci Dis. 2015; 16.
- The difficulties of managing diabetes in Africa. ONG Santé Diabète.
- Sow D, Diédhiou D, Diallo IM, et al. Morbi Infectious Mortality of Diabetics Hospitalized at the Medical Clinic of Abass Ndao Health Center. Open Journal of Endocrine and Metabolic Diseases. 2018; 8: 1-8.