Esophagus Cancer: Epidemiological, Clinical, Para Clinic and Evolving Aspects at Brazzaville Chu
Author'(s): Jile Florient Mimiesse1,2, Ngala Akoa Itoua-Ngaporo1,2, Stéphane Rody Ngami1,2, Clausina Ahoui-Apendi1,2, Arnaud Mongo-Onkouo1,2, Mauria Ibobi2, Bénédicte Ahombo2, Hostaud Atipo Ibara2, Lesty Ibara Kolo2, Pérès Mordoché Motoula Latou1,2, Marlyse Ngalessami Mouakosso2, Deby-Gassaye1,2 and Blaise Irénée Atipo Ibara1,2
1Faculty of Health Sciences of the University Marien Ngouabi Brazzaville, CONGO.
2Department of Gastroenterology and Internal Medicine, University Hospital of Brazzaville, CONGO.
*Correspondence:
Jile Florient Mimiesse, Faculty of Health Sciences of the University Marien Ngouabi Brazzaville, CONGO.
Received: 12 Jan 2022 Accepted: 15 Feb 2022; Published: 21 Feb 2022
Citation: Mimiesse JF, Itoua-Ngaporo NA, Ngami SR, et al. Esophagus Cancer: Epidemiological, Clinical, Para Clinic and Evolving Aspects at Brazzaville Chu. Gastroint Hepatol Dig Dis. 2022; 5(1): 1-3.
Abstract
Introduction: Our study aimed to describe the epidemiological, clinical, paraclinical and evolutionary aspects of esophageal cancer.
Patients and Methods: This is a descriptive retrospective study carried out over 08 years (January 2012 to December 2020) in the gastroenterology and internal medicine department of the Brazzaville University Hospital. We included the files of patients hospitalized for CO retained on a clinical and endoscopic argument bundles.
Results: During the study period, 34 cases of esophageal cancer were diagnosed, ie a hospital frequency of 0.63%. The average age was 52.97 years with extremes ranging from 29-90 years. They are made up of 24 men and 10 women with a sex ratio of 2.4 in favor of men. Alcohol-smoking poisoning was found in 21 male patients with an average of 27 packs / year. The main symptom at diagnosis was dysphagia (55.88%). Esogastroduodenal fibroscopy showed ulcerative budding and hemorrhagic lesions (50%), the site of which was mainly the abdominal esophagus (64.70%). Adenocarcinoma was the most common histologic type, 16 patients received palliative care.
Conclusion: Esophageal cancer is common in males over the age of 50. Dysphagia is the most frequent reason for consultation. The distal esophagus is the most common site of esophageal cancer and the histologic type is adenocarcinoma. Among our patients, 16 received palliative care.
Keywords
Introduction
Esophageal cancer (OC) is a primary malignant tumor that develops at the expense of the lining of the esophagus. It is characterized by its variable incidence depending on the region and by its severity. Indeed, it is one of the deadliest cancers of the digestive tract. His diagnosis is often late. Its unfavorable prognosis is mainly based on the lack of early detection of precancerous lesions due to late consultation of patients as soon as the first symptom appears [1]. Esophageal cancer is the eighth most common cancer and the sixth leading cause of cancer death worldwide [2]. In developing countries, CO is the fifth leading cause of cancer death, and 80% of all mortality occurs in developing countries [3]. In Togo, the hospital frequency of esophageal cancer is 0.55%. In the Congo, rare studies have reported a frequency of esophageal cancer, which represented 2.1% of primary digestive cancers in 2004 [4]. Our objective was to describe the epidemiological, clinical, paraclinical and evolutionary aspects of esophageal cancer in the gastroenterology and internal medicine department at the Brazzaville University Hospital.
Patients and Methods
This is a descriptive retrospective study carried out over 08 years (January 2012 to December 2020) in the gastroenterology and internal medicine department of the Brazzaville University Hospital. We included the files of patients hospitalized for CO retained on a clinical and endoscopic argument bundles. The data were collected from a survey sheet comprising epidemiological, clinical, and endoscopic. Our data was analyzed using Excel starter 2010 software.
Results
During our study period, 5320 patients were hospitalized in the department, 34 of whom fulfilled our inclusion criteria. This corresponds to a hospital frequency of 0.63% of hospitalizations in the department. They are made up of 24 men and 10 women with a sex ratio of 2.4 in favor of men.
The average age of patients is 52.97 years (29-90 years) with a bimodal distribution: 26 patients with an average age of 45.6 years (29-60 years) and 9 patients with an average age of 73.77 years (65-90 years).
Alcohol-smoking poisoning was found in 21 male patients with an average of 27 packs / year. Four patients consumed only alcohol and 9 consumed only tobacco. Three patients consumed hot drinks, there were two cases of Plummer Vinson syndrome, three patients had a history of gastroesophageal reflux, five patients consumed herbal tea daily.
The average time to diagnosis was 3 months with extremes ranging from 1 month to 7 months.
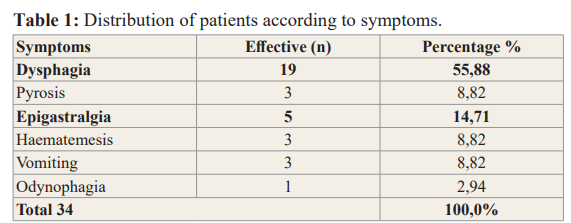
Most patients were admitted for dysphagia n = 19 (55.8%), hematemesis n = 3 (8.2%), heartburn n = 3 (8.2%), odynophagia n = 1 (2.94%), vomiting n = 3 (8.2%) and epigastralgia n = 5 (14.70%). The functional signs have been shown in Table 1.
The clinical examination had noted two cases of Troisier's lymph nodes, 2 cases of hepatomegaly and 4 cases of paleness of the conjunctival mucosa.
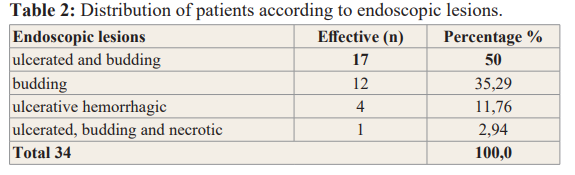
Eso Gastroduodenal endoscopy showed ulcerative budding and hemorrhagic lesions in 17 cases (50%), budding in 4 cases (11.76%), ulcerating buds in 12 cases (35.29%) and ulcerative budding and necrosis in 1 case (2.94%). The stenosis was present in 8 patients (23.52%) and was complete in 3 patients. The lesion was located in the cervical esophagus in 8 cases (23.52%), the thoracic esophagus in 4 cases (11.76%) and the abdominal esophagus in 22 cases (64.70%). Endoscopic lesions are shown in Table 2.
Discussion
The hospital frequency of esophageal cancer was 0.63%. Data from the literature in Africa report low prevalence of esophageal cancer. Indeed, Mâli Koura et al had reported a hospital frequency of 0.62% in Bobo Diolasso [5]. Bouglouga Oumboma in Lomé reported a hospital frequency of 0.55% [6]. On the other hand, the most important prevalence was observed in Niger and Ethiopia respectively of 3.22% and 6.3% [7,8]. The low rates reported in Africa can be explained on the one hand by the fact that a large number of patients are underdiagnosed, on the one hand due to the low accessibility to upper digestive endoscopy in our work context, and on the other hand from poor orientation of patients in otorhinolaryngology for dysphagia.
During our study, the mean age was 52.97 years with a bimodal distribution: 26 patients with a mean age of 45.6 years (29-60 years) and 9 patients with a mean age of 73.77 years (65 -90 years old). Our results are comparable to those of Mâli Koura et al as well as to Jean Paul Ndamba Engbang who found a respective mean age of 58 years and 54 years [5,8]. The sex ratio was in favor of men. This result is similar to that of Tettey et al in Ghana, which shows a male / female ratio of 4.1 [9]. A work by Norderstedt and Séraq, the male / female ratio of esophageal cancer varied by histology, age and race [10].
Tobacco and alcohol play a major role in the development of esophageal cancer. In our study, alcohol-smoking poisoning was found in 21 male patients with an average of 27 packs / year. According to Lin et al, alcoholism and smoking have a synergistic effect in esophageal cancer and the risk depends on the duration of exposure [11]. Wheeler and Redd reported greater carcinogenic activity of tobacco in esophageal cancer for aromatic hydrocarbons in tar and volatile nitrosamines [12]. The mechanism of action of etylism (the risk of which increases with the amount of drinks consumed) remains uncertain and various theories have been proposed, such as irritation of the mucous membranes, increased susceptibility to other carcinogens, in addition to 'a consequent nutritional deficiency [12]. Alcohol can damage cellular DNA by decreasing metabolic activity within the cell and therefore reduce detoxification function while promoting oxidation [13]. Alcohol is a solvent, especially fat-soluble compound. Therefore, the dangerous carcinogens contained in tobacco are able to enter the esophageal epithelium more easily.
Half of the cases in this work were admitted for dysphagia (55.8%) followed by epigastralgia. The consultation time varied between 1 and 7 months after the appearance of the first symptom. Our results can be superimposed on African authors [7,14-16]. This delay could be explained by the fact that a good part of the patients would be underdiagnosed, on the one hand due to the poor accessibility to the upper gastrointestinal endoscopic, and on the other hand to a bad orientation of the patients in Otho-rhinolaryngology for dysphagia.
In 64.70% of cases (n = 22), the endoscopic lesion was located in the abdominal esophagus, followed by the cervical esophagus in 23.52% of cases (n = 8). Certain authors in Africa have made this observation. Indeed Rénovat Ntagirabiri et al in Burundi had reported 55.9% of cases of lesions located in the lower third of the esophagus [17]. The same observation was made by Bagnhy et al in Lomé [18].
The macroscopic appearance was dominated by ulcerative budding lesions in 50% of cases and budding in 35.29% of cases. Our results are similar to those of Thiam et al. in Dakar [19] as well as those of Mâli Koura et al in Burkina faso [5]. On the other hand, Mustapha et al had found ulceration-type lesions that localized ulceration was the most common morphology [20]. In Japan, the most frequent morphologies were the ulcerative type and the infiltrating ulcerated type located in the lower third of the esophagus [21].
Regarding the histological type, adenocarcinoma was found in 65% of cases. Stenosis was present in 8 cases. This observation was made by Harouna Y et al in Niger [7]. On the other hand.
Conclusion
Esophageal cancer is common in males over 50 years of age in the Gastroenterology and Internal Medicine department of the Brazzaville University Hospital.The alcohol-smokingimpregnation is the most common risk factor in our series. Dysphagia is the most frequent reason for consultation. The distal esophagus is the most common site of esophageal cancer and the histologic type is adenocarcinoma.
References
- Faivre Jean, Lepage Côme, Bouvier Anne-Marie. Données récentes sur l’épidémiologie du cancer de l’œsophage. Gastroenterol Clin 2005; 29: 534-539.
- Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, CA Cancer J Clin. 2005; 55: 74-108.
- Pisani P, Parkin DM, Bray F, et Estimates of the worldwide mortality from 25 cancers in 1990. Int J Cancer. 1999; 83: 18-29.
- Peko JF, Ibara JR, Dangou JM, et Profil histo- épidemiologique de 375 cancers digestifs primitifs au chu de Brazzaville. Med Trop. 2004; 64: 168-170.
- Mâli Koura, Roland Ollo Somé, Damien Z Ouattara, et Le Cancer de l’Œsophage à Bobo-Dioulasso (Burkina Faso): Aspects Épidémiologiques, Cliniques, Endoscopiques et Anatomopathologiques. Health Sci. Dis 2020; 21: 21-25.
- Bouglouga O, Lawson-Ananissoh LM, Bagny Aklesso, et al. Etude descriptive et analytique du cancer de l’œsophage au Pan Afr Med J. 2014; 19: 315.
- Harouna YD, Illo A, Assoumane I, et al. Les cancers de l’oesophage au Niger aspects épidémiologiques et cliniques. A propos de 36 cas. Méd Afr 2008; 55: 235-239.
- Jean Paul Ndamba Engbang , Basile Epidemiological and Histopathological Characteristics of Esophageal Cancers in Cameroon. Cancer Research Journal. 2019; 7: 150-156.
- Tettey M, Edwin F, Anitey E, et The changing epidemiology of esophageal cancer in sub-Saharan Africa–the case of Ghana. Pan African Medical Journal. 2012; 13: 6.
- Nordenstedt H, El-Serag H. The influence of age, sex, and race on the incidence of esophageal cancer in the United States (1992-2006). Scand J 2011; 46: 597-602.
- Lin Y, Totsuka Y, He Y, et al. Epidemiology of esophageal cancer in Japan and J Epidemiol. 2013; 23: 233-242.
- Wheeler GB, Reed CE. Epidemiology of esophageal cancer. Surg Clin N 2012; 92: 1077-1087.
- Muwonge R, Ramadas K, Sankila R, et al. Role of tobacco smoking, chewing and alcohol drinking in the risk of oral cancer in Trivandrum, India: a nested case-control design using incident cancer Oral Oncol. 2008; 44: 446-454.
- Maïga YM, Diallo G, Dembélé M, et Cancer de l’oesophage: aspects épidémiologiques, cliniques et pronostiques. Acta Endoscopica. 2002; 32: 455-459.
- Sawadogo A, Ilboudo PD, Durand G, et Epidémiologie des cancers du tube digestif au Burkina Faso: apport de 8000 endoscopies effectuées au centre hospitalier Sanou sourou (CHSS) de Bobo dioulasso. Med Afr Noire. 2000; 47: 342-345.
- Dia D, Bassene ML, Ndiaye-Bâ N, et Aspects endoscopiques du cancer de l’oesophage à Dakar (Sénégal): etudes de 76 observations. Méd Trop. 2011; 71: 286-288.
- Rénovat Ntagirabiri, Richard Karayuba, Gabriel Ndayisaba, et Esophageal Cancer: Epidemiological, Clinical and Histopathological Aspects over a 24- Years Period at Kamenge University Hospital, Bujumbura, Burundi. Open Journal of Gastroenterology. 2016; 6, 106-110.
- Bagny A, Bouglouga O, Djibril AM, et Cancer de l’oesophage : aspect épidémiologique, clinique et histologique au CHU Campus de Lomé (Togo). J. Afr. Hépatol. Gastroentérol. 2012; 6: 24-27.
- Thiam I, Doh K, Dial C, et al. Profils morpho- épidémiologiques des cancers du sujet âgé à Ger Psychol Neuropsychiatr Vieil. 2014; 12: 354-360.
- Mustafa SA, Banday SZ, Bhat MA, et Clinico- Epidemiological Profile of Esophageal Cancer in Kashmir. Int J Sci Stud. 2016; 3: 197-202.
- Han-Yu Deng, Gang Li, Jun Luo. Does oesophageal stenosis have any impact on survival of oesophageal cancer patients? Interact Cardiovasc Thorac Surg. 2018; 27: 384-386.