Experience of Interventional Cardiology At CHU ''Luxembourg'' In Bamako
Author'(s): TOURE M1,2,5, TERRA A W1, DAGNOGO M1, BA HO2,5, FOFANA D1, DIALL A.A1, DIARRA B2, SOW M1,DAFFE S1, THIAM C A1,5, KEITA A1,5, DOUMBIA M4, COULIBALY M1,5, SANGARE A3, DIARRA BI4 , DIAKITE M3,5, COULIBALY SM1, SANKARE H1 , DIARRA MB1,5 and MENTA I2,5
1Cardiology Department, CHU- Megrave;re Enfant, Bamako-Mali
2Cardiology Department, CHU-Gabriel Toureacute;, Bamako-Mali.
3Cardiology Department, CHU-Point G, Bamako-Mali.
4Center Andre FESTOC, Department surgery cardiac of Bamako Mali.
Faculty of Medecine, University Sciences Technic and Technology of Bamako
*Correspondence:
Dr. Mamadou TOURE MD, Cardiology Department, CHU- Megrave;re Enfant, Bamako, Mali.
Received: 10 Sep 2022; Accepted: 12 Oct 2022; Published: 17 Oct 2022
Citation: TOURE M, TERRA A W, DAGNOGO M, et al. Experience of Interventional Cardiology At CHU ''Luxembourg'' In Bamako. Cardiol Vasc Res. 2022; 6(5): 1-4.
Abstract
Introduction: In the recent past, it was not possible to treat coronary disease in Mali due to a lack of technical facilities. All our coronary patients were evacuated to the Maghreb, France or the sub-region to receive adequate care.
In 2019, the opening of an interventional cardiology room at the University Hospital "Luxembourg" and the training of a team has allowed the local management of a good number of Malians and foreigners suffering from coronary pathology. We report here the results of 30 months of activities.
Methodology: We performed a perspective analysis of coronary angiograms and angioplasties performed in our center from September 2019 to February 2022. Clinical, paraclinical including angiographic data were collected and analyzed.
Results: Between September 2019 and February 2022, 670 patients underwent coronary angiography, 262 of whom were followed by angioplasty. Male gender was predominant (72.6%), a sex ratio of 2.62. The mean age was 59 years and the 46-65 age group was the most dominant (50.24%). High blood pressure was the main cardiovascular risk factor (33.8%). Chronic coronary syndrome was the most frequent indication (59.8%) followed by coronary syndromes (38.3%). The radial route was used in 98%. Coronary angiography was pathological in 69%. Multitruncular lesions were predominant (35.5%) followed by monotruncular (32.8%). 39.10% of our patients underwent angioplasty. Complications were minimal (3%) and mortality was 2.03%.
Conclusion: In our developing countries, we are witnessing an epidemiological transition with the decrease in infectious diseases and the emergence of non-communicable diseases, particularly coronary diseases. Their management requires an adequate technical platform, qualified human resources, and multidisciplinary collaboration.
Keywords
Introduction
Mali is a continental country located in West Africa with an area of 1241238 km2. About twenty years ago, rheumatic valvulopathies were the dominant cardiac pathologies in our country. However, in recent years, due to changes in our lifestyles, we have witnessed an explosion of cardiovascular risk factors such as diabetes, high blood pressure, smoking, dyslipidemia and sedentary lifestyle.
This explosion of cardiovascular risk factors is associated with an emergence of non-infectious cardiovascular pathologies, particularly coronary. In the recent past, it was not possible to treat coronary disease in Mali due to a lack of technical facilities. All our coronary patients were evacuated to the Maghreb, France or the sub-region to receive adequate care.
In 2019, the opening of an interventional cardiology room at the University Hospital "Luxembourg" Figure 1 and the training of a team has allowed the local management of a good number of Malians and foreigners suffering from coronary pathology figure 2. We report here the results of 30 months of activities of our service.

Figure 1: Cathlab of CHU Le LUXEMBOURG.
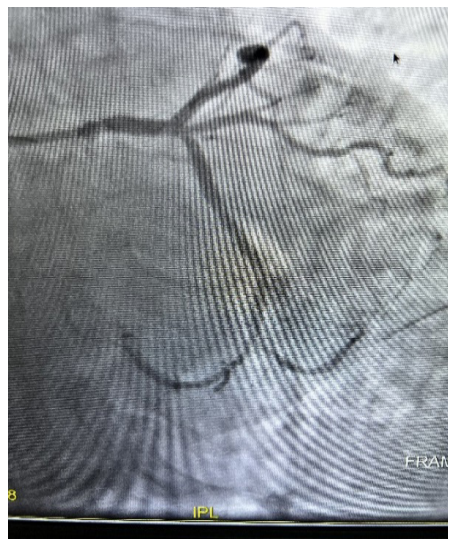
Figure 2a: Befor PCI.
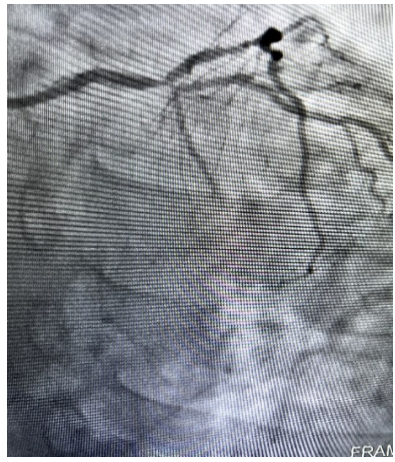
Figure 2b: After PCI.
Methodology
Framework of the study
The cardiology department of the CHU "Luxembourg" is composed of a medical cardiology unit and an interventional cardiology unit called the Mali-Monaco Interventional Cardiology Unit, which served as the study setting.
Patients and Methods
We performed a perspective analysis of coronary angiographies and angioplasties performed in our center from September 2019 to February 2022.
We included all patients who received coronary angiography associated or not with angioplasty. Data were collected on individual survey forms including sociodemographic data, cardiovascular risk factors, history, indications for coronary angiography, coronary angiography procedure, coronary angiography results, angioplasty procedure, complications of coronary angiography and angioplasty procedures. Data analysis was performed with Excel.
Results
Over a period of 30 months, from September 2019 to February 2022, 670 patients had undergone coronary angiography with 262 angioplasties performed in the interventional cardiology unit of the CHU- Luxembourg.
Males predominated (72.6%), with a sex ratio of 2.62.
The mean age was 59 years and the age group 46-65 years was the most dominant (50.24%).
High blood pressure was the main cardiovascular risk factor (33.8%). Chronic coronary syndrome was the most frequent indication (59.8%) followed by acute coronary syndromes (38.3%).
The radial route was used in 98% of cases.
Coronary angiography was pathological in 69%. Multitruncular lesions were predominant (35.5%) followed by monotruncular lesions (32.8%).
Angioplasty was performed in 39.10% of our patients and 0.2% of our patients underwent coronary artery bypass surgery. The stents used were active stents.
Complications were minimal (3%); mortality in the series was 2.03% and was related to the late management of patients.
Discussions
In our series, the mean age was 59 years. This age is close to the 58 years of El Khorb in Morocco, 62 years of Diop in Senegal, and lower than the 68 years of Marcaggi in France. This result confirms that age is a cardiovascular risk factor in our country as elsewhere [1-3].
In our series, as in those in the literature, the male sex was dominant. It was found in 72% of cases in our series, 77% in the series by Diop, 67.8% in that of Larifla4, and 61.3% in that of Jacq [4,5].
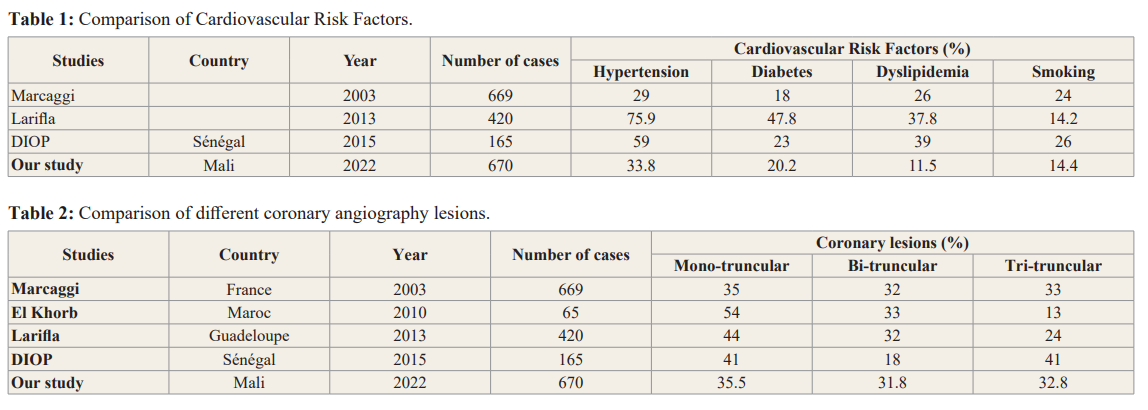
Arterial hypertension was the main cardiovascular risk factor in our series with 33.8%. This result is consistent with those of Larifla and Marcaggi (Table 1).
The radial approach was used in 98% of our series, whereas it was 68% in the Aquitaine registry, 15% in Marcaggi's series, and 33% in Diop's series. The use of the radial approach is associated with a reduction in vascular and hemorrhagic complications, improved patient comfort, faster mobilization and, above all, a reduction in morbidity and mortality [6,7].
In our series, monotruncal involvement was present in 35.5% of cases, bi-truncal in 31.8% of cases and tri-truncal in 32.2% of cases. This result is consistent with that of Marcaggi, who found 35% mono-truncular, 32% bi-truncular and 33% tri-truncular respectively, but also with the rest of the literature Table 2.
Angioplasty was performed in 39.10% of patients with 3% of non- fatal complications, including 1 radial hematoma, 3 compartment syndromes in the arm, 2 recovered cardiac arrests, and 1 ischemic stroke. The patients with compartment syndrome all underwent successful surgical decompression.
Stroke is a rare but dramatic event because of the functional sequelae. In our series it represented 0.4% of the complications. In their series, Werner et al, found 0.3% for stable patients and 0.6% in case of acute coronary syndrome [8].
The mortality in the series was 2.03% and all the patients who died were in cardiogenic shock with tri-truncular lesions. Despite therapeutic advances in recent years, the mortality of patients in cardiogenic shock during infarction remains high. It was of the order of 40-70% in the series of Hollenberg and Hochman [9,10].
Conclusion
Nowadays, we are witnessing an epidemiological transition in our developing countries with the decrease of infectious diseases and the emergence of non-communicable diseases, especially coronary diseases. Their management requires an adequate technical platform, qualified human resources, and multidisciplinary collaboration.
References
- El Khorb. Primary angioplasty in the acute phase of myocardial infarction in the cardiology department of the CHU Hassan II of Fez. Thesis of doctorat in medicine. Fez: Sidi Mohammed Ben Abdellah University. 2011; 84.
- Diop I B. Inaugural experience of interventional cardiology at Jacques Bessol Coronary Angiography Centre of the University Hospital of Fann (Dakar) : Outcomes, difficulties and perspectives. Cardiologie Tropicale. 2017.
- Marcaggi X. Results of percutaneous coronary intervention in a hospital with a case load. Ann Cardiol Angeiol. 2005; 54: 317-332.
- Larifla L. Association between cardiovascular risk factors and coronary lesion severity in Afro-Caribbean subjects. Arch Cardiovasc Dis. 2014; 107: 212-218.
- Jacq L, Chabredier-Paquot, Pezzano M, et al. Valeur pronostic d’une coronarographie Normale. EMC (Editions scientifiques et médicales Elsevier SAS), Ann Cardiol Angéiol. 2001; 50: 404-407.
- Montalescot G, Ongen Z, Guindy R, et al. Predictors of outcome in patients undergoing PCI. Results of the RIVIERA study. Int J Cardiol. 2008; 129: 379-387.
- Pristipino C, Trani C, Nazzaro MS, et al. Major improvement of percutaneous cardiovascular procedures outcomes with radial artery catheterisation: Results from the PREVAIL study. Heart. 2009; 95: 476-482.
- Nicolas Werner, Timm Bauer, Matthias Hochadel, et al. Incidence and clinical impact of stroke complicating percutaneous coronary intervention: results of the Euro heart survey percutaneous coronary interventions registry. Circ Cardiovasc Interv. 2013; 6: 362-369.
- Hollenberg SM, Kavinsky CJ, Parrillo JE. Cardiogenic schock. Ann Inter Med. 1999; 131: 47-59.
- Hochman JS, Sleeper LA, White HD. One year survival following early revascularization for cardiogenic shock. JAMA. 2001; 285: 190-192.