Factors Associated To Diagnostic Delay Of Oromaxillofacial Cancers
Author'(s): Mabika Bredel DD 1,3*, Ngoua Essininguele L1, Faye AD4, Trigo Eboungabeka 1,3, Oball Mond A 1,3 and Ngouoni GC2,3
1Department of Maxillofacial-Aesthetic Surgery and Stomatology,Brazzaville University Hospital.
2Department of otolaryngology and Cervico-facial Surgery,Brazzaville University Hospital.
3Faculty of Health Sciences, Marien Ngouabi University of Brazzaville (Congo).
4Departement of Head and neck surgery, Faculty of Health Sciences,Iba Der Thiam, University, Thiès, Sénégal.
*Correspondence:
Mabika Bredel Djeri Djor. Department of MaxillofacialAesthetic Surgery and Stomatology, Brazzaville University Hospital, Brazzaville, Congo.
Received: 15 May 2023; Accepted: 13 Jun 2023; Published: 18 Jun 2023
Citation: Mabika Bredel DD, Ngoua Essininguele L, Faye AD, et al. Factors Associated To Diagnostic Delay Of Oromaxillofacial Cancers. Cancer Sci Res. 2023; 6(1): 1-4.
Abstract
Introduction: It is not uncommon in developing countries for patients to consult specialists for extended maxillofacial tumours, known as "historic".
Purpose: To identify the socio-demographic and clinical characteristics associated with the delay in establishing the diagnosis of oromaxillofacial cancers in Brazzaville.
Patients and Methods: This was an analytical cross-sectional study with prospective data collection, conducted at the maxillofacial surgery and stomatology department of the Brazzaville Hospital Center, over a period of 24 months from January 2020 to December 2021, out of 37 oromaxillofacial cancers.
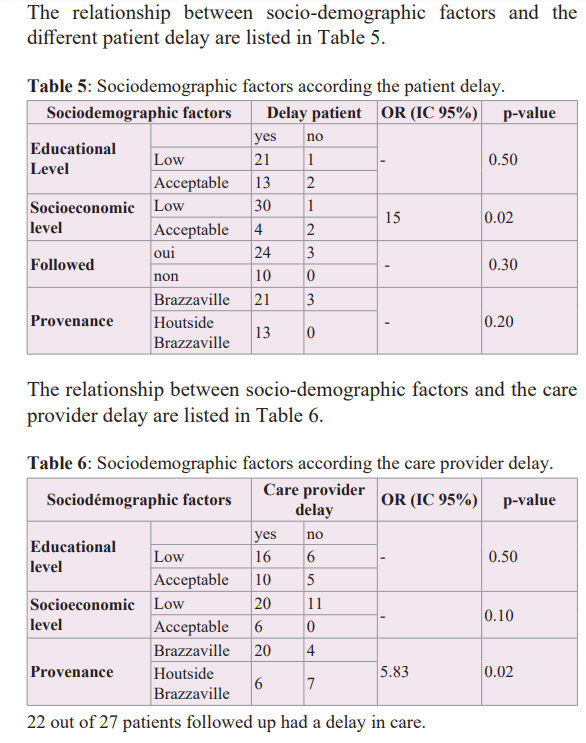
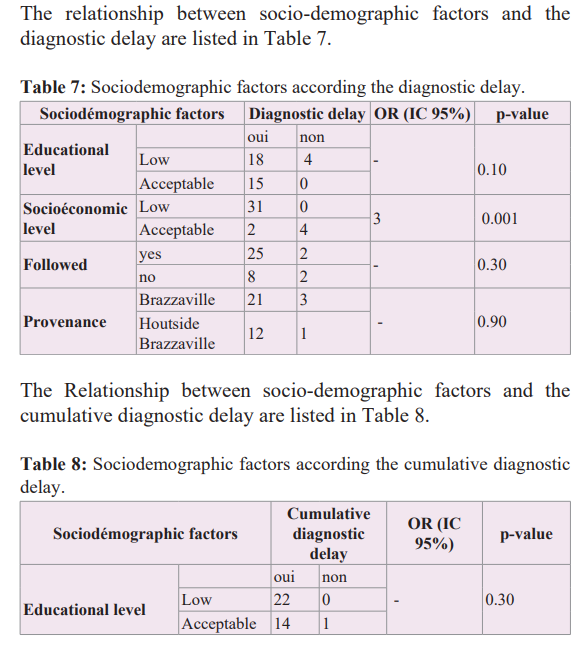
Results: The study involved 37 patients: 23 men and 14 women with a sex ratio of 1.65. The mean age at the time of diagnosis was 45.7±2 years. 79.40% were diagnosed at advanced stages. The diagnostic delay, whether specialized or cumulative, was essentially related to the socioeconomic level (p= 0.04). Those with a low socioeconomic level were 3 times more likely to be diagnosed late than patients with an acceptable socioeconomic level (OR=3). The level of education did not influence the delay (p=0.30).
Conclusion: The responsibility for the delay in diagnosis was found with the patient, the provider of nonspecialized care and the organization of the health system. These delays were influenced by many factors including the low socioeconomic level for all three components, the follow-up by Brazzaville providers for the delay in providing care.
Keywords
Introduction
Early diagnosis and timely initiation of treatment are fundamental to optimize the benefits of treatment for cancers in general and oromaxillofacial cancer in particular [1]. Despite the exposure of the maxillofacial region, symbol of close communication with others, it is not uncommon in developing countries, that patients consult specialists for maxillofacial tumors, with quite long evolution, contributing to extensive tumors called "historicalʺ [2]. This state of affairs, negatively impacts the prognosis [1] and seems to be related to multiple individual factors and in connection with the health care system [3-6].
Several international studies have attempted to quantify the average diagnostic delay and to examine factors that may explain delays in diagnosis after the first symptoms of cancers in general [7].
To our knowledge, no study on the diagnostic delay of oromaxillofacial cancers in the Congo has been published, so it is necessary to understand the factors that influence the diagnostic course of these patients.
Purpose
To identify the sociodemographic and clinical characteristics associated with delay in diagnosis of oromaxillofacial cancers.
Material and Method
We conducted a prospective cross-sectional analytical study in the Department of Maxillofacial Surgery and Stomatology of the Brazzaville Hospital Center, over a 24-month period from January 2020 to December 2021.
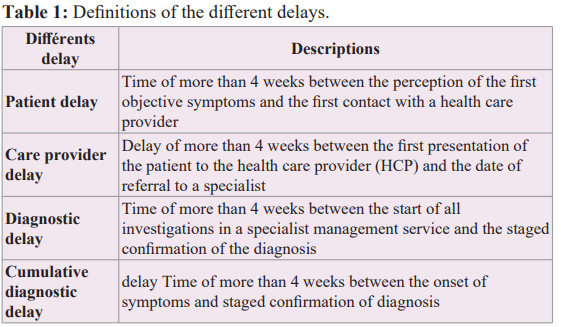
The study population consisted of all malignant oromaxillofacial tumors admitted for consultation during the study period. An individual survey form was the means of data collection by systematic and progressive filling in as soon as the biopsy was obtained. Patients were included by simple random selection. A sample of 37 oromaxillofacial cancers was thus selected and was separated into two groups for each type of delay. Definition of the different delays [3,5,7-9].
The main parameters studied were: age, gender, origin, education level, socioeconomic level, provider profile, different delays, and stage. Statistical tests and p-values were calculated using SPSS version 2.0 with a significance level of 0.05. The order ration (OR) was calculated to assess the association between two binary variables, namely between the different delays and each epidemioclinical parameter, with a 95% confidence interval.
Result
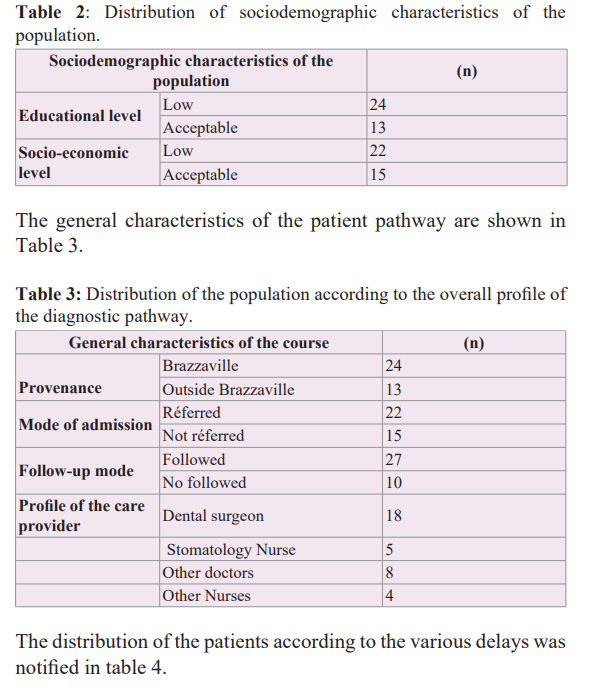
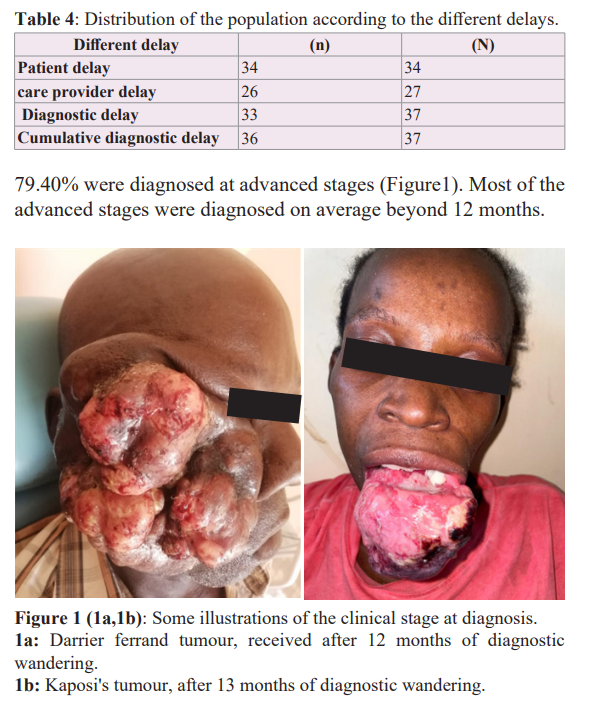
The study included 37 patients : 23 men and 14 women with a sex ratio of 1.65. The mean age at diagnosis was 45.7±2 years. The sociodemographic characteristics of the patients were listed in Table 2.
Discussion
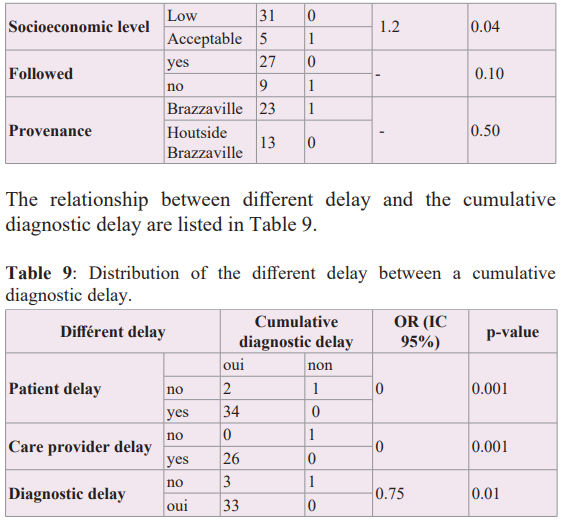
Diagnostic delay, represents an important indicator of the quality of care and performance of the health care system [10-13]. Recently, the concept of delayed diagnosis has become an important issue. The total interval of diagnostic delay has been classified into four components : patient delay, care provider delay, referral delay, and diagnostic delay [7,10,14].
This study, which had some limitations, notably the small sample size and the fact that the health care personnel who consulted the patient before the specialized care was not interviewed to understand their specificity, nevertheless allowed us to identify some factors associated with the delay in diagnosis of oromaxillofacial cancer in Brazzaville.
This study involved a young population, the average age was 45.7±2 years with a slight male predominance, moderately educated, with a relatively low socioeconomic level. This trend of younger and younger cancer patients, low socioeconomic status and male predominance has also been found in many studies [3,6]. This may be explained by exposure to traditional risk factors with probably varying degrees of consumption of foods low in trace elements [7]. Patients (79,40%). were mainly diagnosed at advanced stages beyond (CT3-4).
In spite of their location in a region of exposure, permanently contemplated by others, cancers of the orofacial region are not an exception because they are still diagnosed late in Brazzaville (97.3%).
The delays were noted in all 4 components. Several factors were identified as being associated with diagnostic delay. Patient delay was related to socio-economic level (P= 0.02), those with a low socio-economic level were 15 times more likely to consult late (OR=15). On the other hand, the level of education, the follow-up and the origin did not influence this delay. This could be explained by the fact that poor patients without health insurance would be reluctant to consult health facilities in a timely manner. They may therefore resort to alternative means, notably the contribution of religious or traditional therapists. Delayed access to health care was related to origin (p=0.02). Providers in Brazzaville delayed patients 5.83 times more than those in the interior of the country (OR=5.83). The tendency to want to manage patients without specialist advice would explain this phenomenon. An improvement of our clinical practices through continuous training and interaction between professionals is essential to fight against this phenomenon. The diagnostic delay, whether specialized or cumulative, was primarily related to socioeconomic status (p=0.04). Patients with low socioeconomic status were 3 times more likely to be diagnosed late than patients with acceptable socioeconomic status (OR=3).
The level of education did not influence the delay in diagnosis (p=0.30), as this level does not affect knowledge of the diseases and less so the status guaranteeing the ability to pay for care. These parameters at the origin of the delay in diagnosis have also been found in both developing and developed countries, but in variable proportions [6,15-20].
Conclusion
The oromaxillofacial cancers are still diagnosed late at advanced stages in Brazzaville. The responsibility for the diagnostic delay was found in the patient, the non-specialized care provider and the organization of the health system. These delays were influenced by numerous factors, including the low socioeconomic level for all three components, and the follow-up by Brazzaville providers for the delayed care. This would justify the implementation of the necessary corrective measures, notably to improve patient and caregiver delays through better patient information, improved continuing education for caregivers, the use of interprofessional communication and the promotion of available expertise, without forgetting the facilitation of access to universal health insurance.
References
- Barthélémy, Sannajust JP, Revol P, et al. Cancers de la cavité buccale: préambule, épidémiologie, étude clinique. Stomatologie. ln: Encycl Méd Chir. Paris: Elsevier. 2005.
- Boutault, Paoli JR, Lauwers F. Reconstruction chirurgicale des pertes de substance des maxillaires. EMC-Stomatologie. 2005; 231-253.
- Deepak G, Gita K, Rajan P, et al. “Estimates of delays in diagnosis of cervical, cancer in Nepal,” BMC Womens 2014; 4: 29.
- Prevost V, Joubert C, Heutte N, et Assessment of nutritional status and quality of life in patients treated for head and neck cancer. Eur Ann Otorhinolaryngol Head Neck Dis 2014.
- Teppo H, Olli-Pekka Comorbidity and diagnostic delay in cancer of the larynx, tongue and pharynx Oral Oncol. 2009; 45: 692-695.
- GASSAMA BC. Tabagisme et lésions bucco-dentaires : A partir d’une étude prospective chez des patients tout venant dans un service de santé publique. Thèse : Chir. Dent. Dakar 2000 N° 14.
- Hansen RP, Olesen F, Sørensen HT, et al. “Socioeconomic patient characteristics predict delay in cancer diagnosis: a Danish cohort study,” BMC Health Services Research. 2008; 8: 49.
- Vandborg MP, Christensen RD, Kragstrup JD, et al. “Reasons for diagnostic delay in gynecological malignancies”. International Journal of Gynecological 2011; 21: 967-974.
- Olesen F, Hansen RP, Vedsted P. “Delay in diagnosis: the expérience in Denmark,” British Journal of Cancer. 2009; 101: S5–S8.
- Gyenwali D, Pariyar J, Onta “Factors associated with late diagnosis of cervical cancer in Nepal,” Asian Pacific Journal of Cancer Prevention. 2013; 7: 4373-4377.
- Trussler T. Uncovering the Gaps: An Inquiry of Breast Care in British Columbia, Canadian Breast Cancer Foundation, Vancouver, Canada. 20014.
- Timothy PH, Will DK, Stephane T, et al. Mortalité due au retard de traitement du cancer: revue systématique et méta- analyse. BMJ. 2020; 371: 4087.
- Gorey KM, Luginaah IN, Holawaty EJ, et al. Wait times for surgical and adjuvant radiation treatment of breast cancer in Candada abd United State: greater socioéconomic inequity in America. Clin Investing Med Clin Exp. 2009; 32: E239.
- Cancer Reform Strategy [Internet]. United Team; 2007 déc [cité 25Aout 2015. Disponible sur: http://www.nhs./NHSEngland/NSF/Documents/Cancers%Reform%20Strategy.pdf.
- Kowalski LP, Carvalho AL. Influence of time delay and clinical upstaging in the prognosis of head and neck cancer Oral Oncol. 2001; 37: 94-98.
- Mackillop WJ, Bates JH, O'Sullivan B, et al. The effect of delay in treatment on local control by radiotherapy Int J Radiat Oncol Biol Phys. 1996; 34: 243-250.
- Marre A, Baies M. Délai de prise en charge en cancérologie: Chemin clinique et place du programme personnalisé de soins : obsession? nécessité? contrainte? France: CHU Jaques-Puel, Rodez. 2011; 730: 1-7.
- Rutqvist LE. Waiting times for cancer patients – a « slippery slope » in oncology. Acta Oncol. 2006; 45: 121-123.
- Guyatt GH, Sackett DL, Sinclair JC, et Users’guides to the medical literature. IX. A method for grading health care recommendations. Evidence-Based Medicine Working Group. JAMA. 1995; 274: 1800-1804.
- The Canadian Task Force on the Periodic Health The periodic health examination. Can Med Assoc J. 1979; 121: 1193-254.