Familial Hypercholesterolemia with Multiple Large Tendinous Xanthomas, Severe Aortic Stenosis and Coronary Atherosclerosis in a Young Man: A Case Report from Sénégal
Author(s): Fatou Aw1*, Leye Mohamed2, Mingou Joseph3, Sarr Simon Antoine1, Affangla DA2, Bodian Malick1, Ndiaye Mouhamadou Bamba1, Mbaye Alassane3, Kane Adama1, Diao Maboury1, Kane Abdoul5, Ba Serigne Abdou1
1Department of Cardiology/ Faculty of Medicine, Pharmacy and Odontostomatology, University Cheikh Anta Diop of Dakar/ Teaching Hospital Aristide Le Dantec, Dakar, Senegal.
2Department of Cardiology/ UFR of Health Sciences, University of Thies/ Teaching Hospital of Fann, Dakar, Senegal.
3Department of Cardiology/ Faculty of Medicine, Pharmacy and Odontostomatology, University Cheikh Anta Diop of Dakar/ General Hospital of Grand Yoff, Dakar, Senegal.
4Department of Cardiology/ Faculty of Medicine, Pharmacy and Odontostomatology, University Cheikh Anta Diop of Dakar/ Teaching Hospital of Fann, Dakar, Senegal.
5Department of Cardiology/ Faculty of Medicine, Pharmacy and Odontostomatology, University Cheikh Anta Diop of Dakar/ University Polyclinic, Dakar, Senegal.
*Correspondence:
Fatou Aw Leye, MD, Department of Cardiology/ Faculty of Medicine, Pharmacy and Odontostomatology, University Cheikh Anta Diop of Dakar/ Teaching Hospital Aristide Le Dantec, Dakar, Senegal.
Received: 17 January 2020; Accepted: 05 February 2020
Citation: Fatou Aw, Mingou Joseph, Leye Mohamed, et al. Familial Hypercholesterolemia with Multiple Large Tendinous Xanthomas, Severe Aortic Stenosis and Coronary Atherosclerosis in a Young Man: A Case Report from Sénégal. Cardiol Vasc Res. 2020; 4(1); 1-5.
Abstract
Background: FH is characterized by increased level of serum low-density lipoprotein (LDL) cholesterol with a high prevalence of coronary atherosclerosis.
Case Presentation: We herein present a case of a Familial hypercholesterolemia in a 18 years old patient with severe aortic stenosis and coronary artery atherosclerosis. In its antecedent a family history of dyslipidemia, the patient was diagnosed as having familial hypercholesterolemia. He had hypercholesterolemia and presented with multiple large tendinous xanthomas. Transthoracic echocardiogram finds a severe aortic stenosis, Coronary angiography showed severe multivessel coronary artery stenosis with left main coronary artery stenosis and a severe stenosis in the right coronary artery ostium. Genetic test indicates but was unfortunately not performed to identify the gene mutations responsible for the phenotype. The patient was placed on a statin with dietary modification. Replacement of his aortic valve with coronary artery bypass graft surgery was preconized.
Keywords
Introduction
Familial hypercholesterolemia (FH) is an autosomal inherited disorder caused by mutations in the LDL receptor (LDLR) gene, the apolipoprotein B (APOB) gene, or the proprotein convertase subtilisin/kexin type 9 (PCSK9) genes [1]. FH is characterized by increased level of serum low-density lipoprotein (LDL) cholesterol with a high prevalence of coronary atherosclerosis. It may be inherited as an autosomal dominant trait, and the frequencies of homo- and heterozygotes are estimated to be 1/1×106 and 1/500, respectively, in the general population [2]. Xanthomas are a characteristic feature of FH and most usually measure a few centimetre’s in diameter [2]. It has been reported that the presence of xanthomas increases the risk of cardiovascular disease in FH patients by as much as three times, suggesting that xanthomas and atherosclerosis may share a certain etiology [2]. If left untreated the disease, can lead to premature coronary heart disease, vascular calcifications, and valvularand supravalvar aortic stenosis [3]. In patients who are homozygous for FH, the prevalence of Aortic valves calcifications reaches 100%, and surgical intervention of functional valvular disease is often needed [3]. We herein present a case of a Familial hypercholesterolemia in an 18 years old patient with severe aortic stenosis and coronary artery atherosclerosis.
Case Presentation
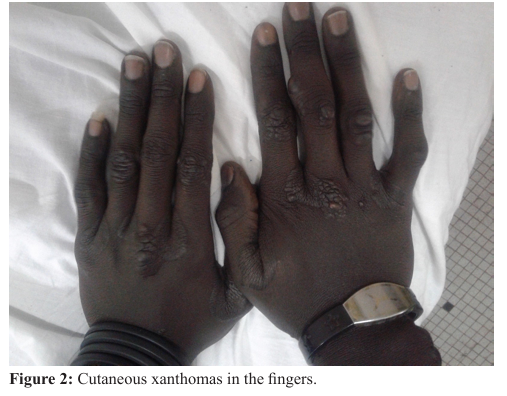
Mr MN, 18 years old, received for stage III of NYHA dyspnea with stage II dyspnea and a cough with whitish sputum, no orthopnea, no chest pain or fever. In his family history there was a known little brother with xanthomatosis who died in childhood and he would carry the same disease for which he has been followed since he was young. The patient also reported two episodes of syncope to major efforts, the first in one-year ago and the last in less than 6 months. The examination found: a blood pressure of 100/80 mmHg, a heart rate of 112 beats /min, a weight of 59 kg for a height of 1.69 m, an apyrexia. Auscultation, found regular tachycardia the perception of a systolic murmur irradiated in neck vessel (intensity 4/6). The lung auscultation was free, there was no spontaneous turgescence of the jugular veins. The remainder of the examination revealed nodular compartments disseminated to the fourth limbs, predominating next to the joints, painless, non-pruriginous existing since childhood corresponding to xanthomatoses (Figures 1 and 2).

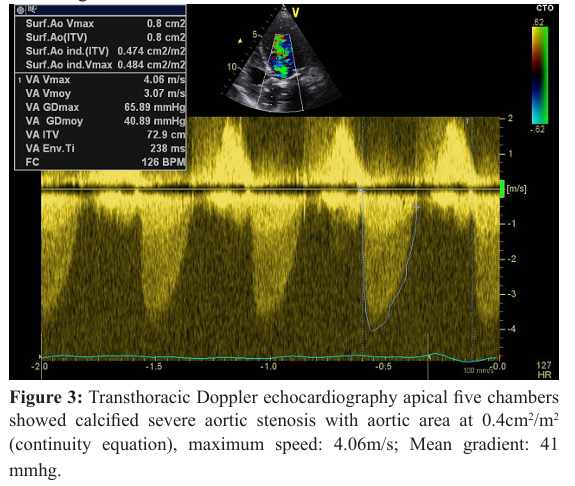
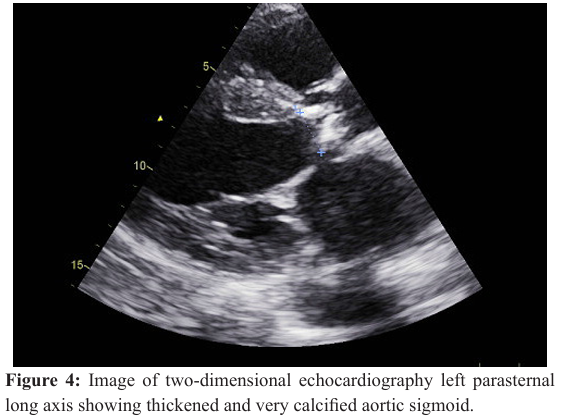
The ophthalmologic examination found xanthelasma of the internal angle of the right eye, another xanthelasma of the external angle of the left eye, and gerontons of both eyes, there was no cataract. At the biology the hemogram, fasting glucose, blood ionogram, serum creatinine, and blood urea were normal. There was a disturbance of the lipid profile with a cholesterol level of 382 mg/dl, an LDL at 353 mg/dl, a HDL (high-density lipoprotein) at 14 mg/dl and triglycerides at 72 mg/dl. The electrocardiogram recorded a regular sinus tachycardia at 119 cycles / min, a QRS axis at + 70â?¦, left atrial hypertrophy, diastolic left ventricular hypertrophy, and anterosal septal R abrasion. The chest X-ray showed cardiomegaly (65% cardiothoracic index) and bilateral hilar overload. Transthoracic Doppler echocardiography showed calcified severe aortic stenosis with aortic area at 0.3 cm² (continuity equation), maximum speed:6.09 m/s; Mean gradient: 92 mmhg (Figure 3), the initial aorta and descending aorta were small with aortic area at 0.4 cm2/m2 (continuity equation), maximum speed: 4.09 m/s; Mean gradient: 40 mmhg.
There was significant repercussion on the left ventricle, which was enlarged with mean systolic dysfunction (left ventricular ejection fraction at 38% in Simpson biplane), moderate to severe mitral insufficiency by dilatation of the mitral annulus, average tricuspid insufficiency with severe pulmonary hypertension Systolic pulmonary arterial pressure at 97mmHg, a moderate circumferential pericardial effusion with no sign of poor tolerance. There was no valvular vegetation. Before this symptomatic severe aortic stenosis on familial dyslipidemia with persistence of a contractile reserve (average Gradient at 92mmHg), a coronarography was performed for this patient. Coronary angiography showed severe multivessel coronary artery stenosis with left main coronary artery stenosis and severe stenosis in the right coronary artery ostium. From a medical point of view the patient was on a diet low in saturated and polyunsaturated fats, rosuvastatin 80mg per day, Aspirin 100mg per day, furosemide 80mg per day. We preconized a double coronary bypass and aortic valve replacement with plasty on the mitral valve. Unfortunately, in the absence of financial support the surgery was not done. The patient presented 6 months later refractory heart failure and died.
Discussion
The frequency of clinical FH is estimated at 1 per 1 000 000, although higher frequencies have been reported in specific populations including French Canadians, Afrikaners in South Africa, and Christian Lebanese [3]. Genetic studies have identified lipoprotein (a) (Lp (a)) as a risk factor for aortic calcification and progressive aortic stenosis [3]. Lp (a) levels have been shown to be elevated in Homozygote FH [3], however the Lp (a) level was not obtained in our patient; Generally, the patients present early in life with cutaneous xanthomas [3], such as in our case. Xanthomas are a characteristic feature of FH and most usually measure a few centimeters in diameter [4]. Multiple large tendinous xanthomas and advanced coronary artery atherosclerosis were noted in the present case. It has been reported that the presence of xanthomas increases the risk of cardiovascular disease in FH patients by as much as three times, suggesting that xanthomas and atherosclerosis may share a certain aetiology [5].
The formation of Aortic Valve Calcification may be related to osteoblast-like cells in the vascular smooth muscle, but the origin of the cells is controversial [6,7]. A recent study by Smith et al. [8] using Mendelian randomization found that a genetic predisposition to elevated LDL was associated with the presence of Aortic Valve Calcification and the incidence of functional aortic stenosis in large community-based cohorts. In a European study, computed tomography detected aortic valve calcification in 38% FH patients [9]. Groups of researchers have demonstrated that cholesterol levels and duration after diagnosis of FH are associated with aortic stenosis [10,11]. However, the relation between cholesterol exposure and aortic stenosis in FH is not consistent among studies [12].
The standard medical therapies include dietary modification in combination with pharmacotherapy (eg statins, ezetimibe, bile resins) and lipid apheresis to lower LDL [3]. Liver transplant is often reserved for severe cases [3]. A study in FH patients in the United Kingdom showed that lipid-lowering therapy reduced cardiovascular risk by 24%-48% [13]. Furthermore, the relative risk reduction by lipid management was up to 76% in another study [14]. In the future, novel therapeutic agents may improve prognosis in FH patients. Recently, clinical trials using emerging pharmacological agents, including a proprotein convertase subtilisin–kexin type 9 (PCSK9) inhibitors, were performed in FH patients. PCSK9 inhibitors have shown tremendous and consistent LDL lowering efficacy with acceptable tolerability and seem to be the most promising among new therapeutic options [15].
Conclusion
Familial hypercholesterolemia is a disorder that is caused LDL cholesterol level to be very high. These disorders caused a high risk of atherosclerosis with possibility of coronary desease and sudden cardiac death.
References
- Gert-Jan R Ten Kate, Sven Bos, Admir Dedic, et al. Increased Aortic Valve Calcification in Familial Hypercholesterolemia: Prevalence, Extent, and Associated Risk Factors. J Am Coll Cardiol. 2015; 66 : 2687-2695.
- Terasaki F, Morita H, Harada-Shiba M, et al. Familial Hypercholesterolemia with Multiple Large Tendinous Xanthomas and Advanced Coronary Artery Atherosclerosis. Intern Med. 2013; 52: 577-581.
- Greco M, Robinson JD, Eltayeb O, et al. Progressive Aortic Stenosis in Homozygous Familial Hypercholesterolemia After Liver Transplant. Pediatrics. 2016; 138.
- Weiss SW, Goldblum JR. Soft Tissue Tumors. 5th ed. Mosby Elsevier, Philadelphia. 2008; 355-358.
- Daniëlla M Oosterveer, Jorie Versmissen, Mojgan Yazdanpanah, et al. Differences in characteristics and risk of cardiovascular disease in familial hypercholesterolemia patients with and without tendon xanthomas: a systematic review and meta-analysis. Atherosclerosis. 2009; 207: 311-317.
- Awan Z, Alrasadi K, Francis GA, et al. Vascular calcifications in homozygote familial hypercholesterolemia. Arterioscler Thromb Vasc Biol. 2008; 28: 777-785.
- Fantus D, Awan Z, Seidah NG, et al. Aortic calcification: Novel insights from familial hypercholesterolemia and potential role for the low-density lipoprotein receptor. Atherosclerosis. 2013; 226: 9-15.
- Smith JG, Luk K, Schulz CA, et al. Association of low-density lipoprotein cholesterol-related genetic variants with aortic valve calcium and incident aortic stenosis. JAMA. 2014; 312:1764-1771.
- Vongpromek R, Bos S, Ten Kate GJ, et al. Lipoprotein(a) levels are associated with aortic valve calcification in asymptomatic patients with familial hypercholesterolaemia. J Intern Med. 2015; 278: 166-173.
- Rallidis L, Naoumova RP, Thompson GR, et al. Extent and severity of atherosclerotic involvement of the aortic valve and root in familial hypercholesterolaemia. Heart. 1998; 80: 583-590.
- Nozue T, Kawashiri MA, Higashikata T, et al. Cholesterol-years score is associated with development of senile degenerative aortic stenosis in heterozygous familial hypercholesterolemia. J Atheroscler Thromb. 2006; 13: 323-328.
- Summers RM, Andrasko-Bourgeois J, Feuerstein IM, et al. Evaluation of the aortic root by MRI: insights from patients with homozygous familial hypercholesterolemia. Circulation. 1998; 98: 509- 518.
- Neil A, Cooper J, Betteridge J, et al. Reductions in all- cause, cancer, and coronary mortality in statin-treated patients with heterozygous familial hypercholesterolaemia: a prospective registry study. Eur Heart J. 2008; 2625-2633.
- Versmissen J, Oosterveer DM, Yazdanpanah M, et al. Efficacy of statins in familial hypercholesterolaemia: a long term cohort study. BMJ. 2008; 337: a2423.
- Sang-Hak Lee. Characteristics and Vascular Complications of Familial Hypercholesterolemia in Korea. J Atheroscler Thromb. 2016; 23: 532-538.