Giant Myxoma of the Right Atrium a Rare Location: A Case Report at the Festoc Center in Bamako
Author'(s): Diarra B I1*, Doumbia M1, Coulibaly B1-3, Daffe S1, Coulibaly B1, Doucoure O1, Koita S1, Diallo B1, Traore S1, Coulibaly M1, Keita A2, Toure M2-3, Diarra M B2, Togola B2, Togo S2, Ouattara M A2 and Yena S2
1Cardio-Pediatric Andre Festoc Center, Mother-Child Hospital Luxembourg, Mali.
2Department of Cardiology, Mother-Child Hospital Luxembourg Bamako, Mali.
3Faculty of Medicine and Odontostomatology, University of Technical Sciences and Technologies of Bamako, Mali.
*Correspondence:
Dr Baba Ibrahima DIARRA, cardio-vascular and thoracic surgeon, Phone number: 00 223 93 33 63 96.
Received: 11 Apr 2023; Accepted: 13 May 2023; Published: 18 May 2023
Citation: Diarra BI, Doumbia M, Coulibaly B, et al. Giant Myxoma of the Right Atrium a Rare Location: A Case Report at the Festoc Center in Bamako. Cancer Sci Res. 2023; 6(1): 1-3.
Abstract
Right ventricular myxoma is a very rare location of cardiac myxomas. The most common complications are pulmonary embolism and tumor obstruction of the pulmonary valve.
We report the case of a 63-year-old woman admitted to Cardiology for recurrent syncope and progressively worsening dyspnea. Echocardiography revealed right atrial myxoma. Surgical excision was performed under extracorporeal circulation, with favorable postoperative outcomes. Histological examination of the specimen confirmed the diagnosis of myxoma. The 2-month follow-up does not show any tumor recurrence.
Keywords
Introduction
Primary tumors of the heart are rare, their incidence varies from 0.0017 to 0.33% according to different autopsy studies [1]. 75% of them are benign tumors and among them 50% are myxomas [1,2]. Myxoma is observed at any age, with a predominance between 30 and 60 years and an average age between 45 and 50 years [3,4]. This disease is most often discovered incidentally. When it is symptomatic, it is revealed by signs of heart failure or thromboembolic complications. Positive diagnosis is made by echocardiography. Surgical management of this condition using cardio-pulmonary bypass improved its prognosis. This surgery remains indicated in all cases to avoid the occurrence of complications [5].
Case Report
We report the case of a 67-year-old patient known to be hypertensive under treatment who underwent emergency surgery following the fortuitous discovery of a mass in the right atrium during a check-up for stage 2-3 dyspnoea. NYHA, progressively worsening and lower extremity edema (OD). The chest x-ray showed cardiomegaly with a cardio thoracic index of 0.65.
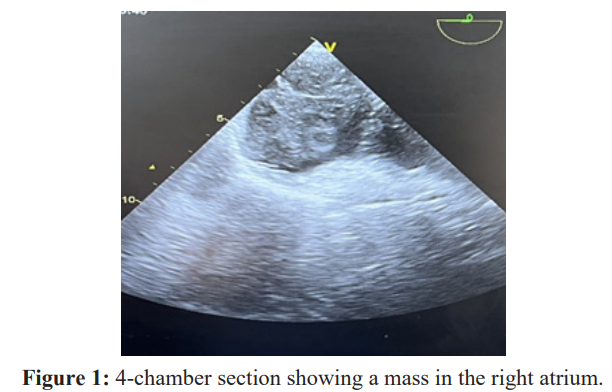
At the electrocardiogram the rhythm was sinus and regular. The Echocardiography showed a tumor in the right atrium: 53.3/70.5 mm, ejection fraction: 47.17% (Figure 1).
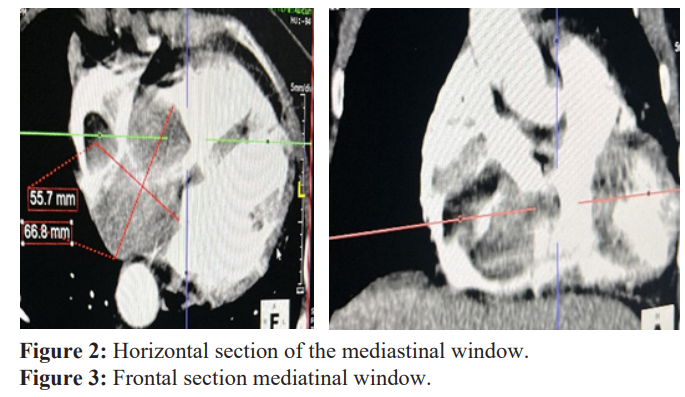
The thoracic CT angiography had revealed a bulky mass not taking the contrast and which prolapsed in the right ventricle (Figures 2, 3).
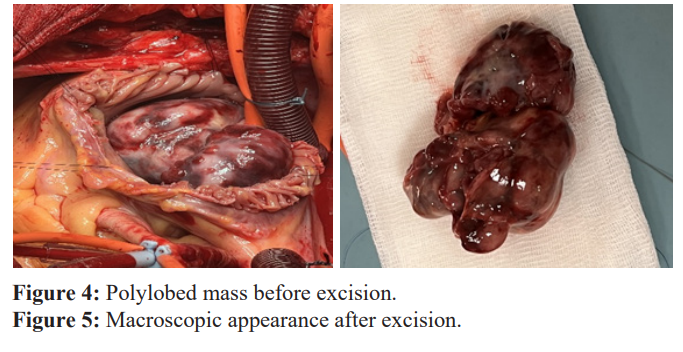
She underwent surgical excision. The approach was a vertical median sternotomy. A cardio-pulmonary bypass was set up, in normothermia, between the ascending aorta and the two vena cava. An approach, by a right atriotomy, made it possible to highlight a polylobed spheroid tumor mass of approximately 6 cm in long axis, which originated from a wide pedicle on the lateral face of the right atrium (Figures 4, 5).
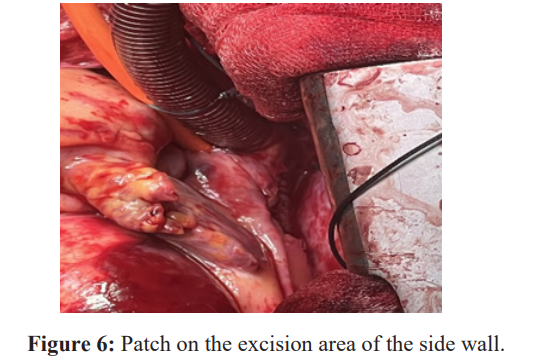
The tumor is resected, removing the lateral wall of the right atrium, which will be repaired by placing a patch of heterologous pericardium (Figure 6).
A Control by intraoperative transesophageal echocardiography shows a right ventricle outflow chamber free of any residual mass, as well as the competence of the pulmonary and tricuspid valves. The postoperative evolution was favorable. The anatomopathologic study of the surgical specimen confirmed the diagnosis of myxoma. Ultrasound follow-up at 2 months postoperatively showed no tumor recurrence [6,7].
Discussion
Myxomas are the most common cardiac tumors [8,9]. In the vast majority of cases, they are located in the atrium, especially the left atrium [10]. The average age of revelation of this pathology is 50 years [11]. Our patient was 63 years old. Exceptionally, cases of diagnosis of cardiac myxoma have been made in the neonatal and prenatal period at 23 weeks of gestation and then operated on 20 days after birth [12].
A female predominance is found by several authors Denguir et al. [13], Muthubaskaran et al. [14] in an Indian series of 32 patients collected over 21 years found 59.3% women. Only Burke's series [15] carried out within the strongly male-dominated American army objectified a male predominance.
The vast majority of myxomas are of single location, multiple locations are more frequently found in familial forms which constitute less than 10% of myxomas [9,11].Localization in the left atrium is the most common in the literature. It is found eight times out of ten.
Muthubaskaran et al. [14] found left atrial localization in 72.2% of their patients.
The right location of a myxoma should also encourage special management of the patient, as in recurrent myxomas where we must look for associative syndromes, such as NAME syndrome (naevi, atrial myxoma, myxoid fibroma, ephelide), LAMB syndrome (lentigines, atrial myxoma, mucocutaneous myxoma, blue naevi), or the Carney complex, including in particular mucocutaneous lentiginosis [13-15]. The patient in our observation does not seem to belong to any of these syndromes. It is therefore, a priori, an isolated myxoma of the right atrium, without associative character.
Once the diagnosis is suspected on ultrasound, surgery must be undertaken urgently because of the high frequency of embolic events (30% of cases) [11]. The excision must be done in one block in order to avoid emboli of tumor fragments. Electrocoagulation of the base of myxoma implantation and excision of part of healthy endocardium seems to prevent recurrence [12]. In our case, we resected the implantation base of the tumor then a patch of pericardium was sutured at the level of the resection area.
In the event of extension to the pulmonary artery or suspicion of pulmonary embolism, exploration of the pulmonary artery should be performed with a view to embolectomy [12]. Currently, surgery using cardio pulmonary bypass remains the treatment of choice for cardiac myxomas and operated patients benefit from a survival equivalent to that of the general population [10]. Nevertheless,long-term ultrasound follow-up must be rigorous, in order to detect any recurrences early, especially in young patients [8].
Conclusion
Myxoma is the most common primary cardiac tumor. Its natural evolution can be entangled with complications, such as thromboembolic accidents or sudden death. Its location in the right atrium is rare. Surgical excision, the only therapeutic option, has a good prognosis. In the long term, the evolution is most often favorable; nevertheless recurrence remains possible, justifying ultrasound monitoring.
References
- Dang CR, Hurley Contralateral Recurrent Myxoma of the Heart. Ann Thorac Surg. 1976; 21: 59-62.
- Gerbode F, Kerth WJ, Hill Surgical management of tumors of the heart. Surg. 1967; 61: 94-101.
- Pavlides G, Levin R, Hauser Left ventricular recurrence of a resected left atrial myxoma. Am Heart J. 1989; 117: 1390-2.
- Rathore K, Hussenbocus S, Stukils R, et Novel Strategies forRecurrent Cardiac Myxoma. Ann Thorac Surg. 2008; 85: 2125-6.
- Hoffmeier A, Sindermann JR, Scheld HH, et Cardiac tumors-diagnosis and surgical treatment. Dtsch Arztebl Int. 2014; 111: 205-11.
- Reynen Cardiac myxomas. N Engl J Med. 1995; 333:1610-72.
- Attar MN, Sharman DC, Al-Najjar Y, et al. A rare case of multiple right heart Intern J Card. 2007; 31; 118 :66-7.
- Mitropoulos F, Giannakoulas G, Kallifatidis A, et al. Right ventricular myxoma in a patient with tetralogy of International Journal of Surgery Case Reports. 2014; 5: 1058-60.
- Lepillier A, Chaib A, Bouguoin W, et Volumineux myxome de l’oreillette droite révélé par une insuffisance cardiaque congestive. Annales de Cardiologie et d’Angéiologie. 2010; 59: 37-39.
- Mishra A, Shah M, Sharma P, et Operative management of intracardiacmyxomas: a single center experience. Medical Journal Armed Forces India. 2014; 70: 5-9.
- Furber A, Prunier F, Laporte J, et Tumeurs cardiopéricardiques. Encycl Med Chir (Elsevier, Paris), Cardiologie-Angéiologie. 1999; 11: 028-A 10.
- McCarthy PM, Jeffrey MP, Schaff HF, et al. The significance of multiple, recurrent, and “complex” cardiac myxomas. J Thorac Cardiovasc Surg. 1986; 91: 389-96.
- Denguir R, Dhiab M, Meddeb I, et Les myxomes cardiaques. Prise en charge chirurgicale. À propos de 20 cas. Ann Cardiol Angeiol. 2006; 55: 49-54.
- Muthubaskaran V, Anitha S, Chandrasekar P, et al. Cardiac myxomas-22 years single center experience. Indian J Thorac Cardiovasc 2010; 26: 239-242.
- Burke AP, Virmani Cardiac myxoma. A clinicopathologic study. Am J Clinpathol. 1993; 100: 671-80.