Hypertensive Heart Disease, Epidemiological, Diagnostic and Evolutionary Aspects: About 103 Cases in a Cardiology Department of Sikasso Hospital in Mali
Author'(s): Traore Abdoulaye Kissima1, Sangaré Zoumana1,2, Doumbia Modibo1, Mingou Joseph Salvador2*, Traore Ousmane1, Birwe Leon1, Traore Salia1, Dioma Elie1, Sanogo Drissa1, Bodian Malick2 and Kane Adama3
1Department of Cardiology, Regional Hospital of Sikasso, Sikasso, Mali.
2Department of Cardiology, Teaching Hospital Aristide Le Dantec, Dakar, Senegal.
3Department of Cardiology, Regional Hospital of Saint Louis, Saint Louis, Senegal.
*Correspondence:
Joseph Salvador Mingou, Cardiology Department, Aristide Le Dantec Hospital University, Dakar, Senegal, Email: mingoujoseph@gmail.com.
Received: 22 November 2018; Accepted: 18 December 2018
Citation: Traore Abdoulaye Kissima, Sangaré Zoumana, Doumbia Modibo, et al. Hypertensive Heart Disease, Epidemiological, Diagnostic and Evolutionary Aspects: About 103 Cases in a Cardiology Department of Sikasso Hospital in Mali. Cardiol Vasc Res. 2018; 2(4): 1-4.
Abstract
Introduction: Hypertensive heart disease is a complication of uncontrolled high blood pressure. It affects 0.7% of the world's population and is the leading cause of death due to high blood pressure.
Objectives: Determine the prevalence and study the epidemiological, diagnostic and progressive aspects of hypertensive heart disease.
Patients and methods: This was a descriptive cross-sectional study over a two-year period (July 1st, 2014 to June 30th, 2016) in the Cardiology Department of Sikasso Hospital for any patient hospitalized for hypertensive heart disease.
Results: One hundred and three patients were selected, representing a hospital prevalence of 7.21%. The mean age of the population was 52 years (15-82 years) with a male predominance (63%) and a sex ratio of 1.7. Smoking was the most common cardiovascular risk factor associated with high blood pressure (71.7%). High blood pressure grade III according to the World Health Organization classification was found in 52.4%. The electrocardiogram showed isolated left ventricular hypertrophy in 89.3% of patients and associated with atrial fibrillation in 9.7%. Doppler echocardiography showed an altered left ventricular ejection fraction (less than 45%) in 58.25% of cases and left ventricular hypertrophy in all patients with a predominance of the concentric type (52.9%). Therapeutically, diuretics and conversion enzyme inhibitors were used in 73.7%, beta-blockers in 17.3% and calcium channel blockers in 9%. Complications were dominated by congestive heart failure (52%), arrhythmia (21%), ischemic stroke (4%). The average length of hospitalization was 5 days. The mortality rate was 1.97%.
Conclusions: Hypertensive heart disease is a common complication of high blood pressure. The prognosis depends on screening and proper management of the scourge of high blood pressure.
Keywords
Introduction
Hypertensive heart disease is a complication of uncontrolled high blood pressure (hypertension). It is estimated that about one billion people worldwide suffer from hypertension and this figure is expected to increase further as the population ages [1].
In Africa, its prevalence is estimated at 21.5% in Abidjan in Ivory Cost and 41% in Ibadan in Nigeria [2]. In Mali, it ranks first among cardiovascular diseases with a prevalence of 37% and represents 43.9% of the reasons for cardiovascular consultation in cardiology [3].
In addition to its high prevalence and potential morbidity, hypertension is the most common cause of left ventricular pressure overload, initially responsible for left ventricular hypertrophy (LVH) and later dilation and heart failure [4]. Hypertensive heart disease is the leading cause of death due to high blood pressure and affects 0.7% of the world population [4]. In the West, hypertensive heart disease has become rare since the advent of new modern antihypertensive molecules [5].
On the other hand, in sub-Saharan Africa its prevalence is estimated at 37.7% in Senegal [6] and 45.9% in Congo Brazzaville [7]. In Mali, its prevalence is estimated at 41.3% [8].
The prognosis for hypertensive heart disease depends on early detection and proper management of hypertension [4].
Objectives
General
Study hypertensive heart disease in the cardiology department of Sikasso Hospital.
Specific
- Determine the prevalence of hypertensive heart disease.
- Describe the different electrocardiographic and echocardiographic anomalies.
- Describe the evolutionary aspects of hypertensive heart disease.
Patients and methods
This was a descriptive cross-sectional study over a two-year period from July 1st, 2014 to June 30th, 2016 in the Cardiology Department of Sikasso Hospital in any patient hospitalized for hypertensive heart disease. The diagnosis was based on the notion or presence of high blood pressure and signs of heart failure.
The parameters studied included epidemiological, clinical, paraclinical, therapeutic and progressive data. Data were collected on a pre-established survey sheet, transcribed into a database and entered using the EXCEL table software version 2010.
The statistical analysis of the data was performed by the SPSS software version 20.0.
The significance threshold had been set as traditionally at p ≤ 0.05.
Results
One hundred and three patients were selected, representing a hospital prevalence of 7.21%.
Radiography of the frontal chest showed cardiomegaly in 80.6% of cases. The electrocardiogram showed isolated left ventricular hypertrophy in 89.3% of patients and associated with atrial fibrillation in 9.7%.
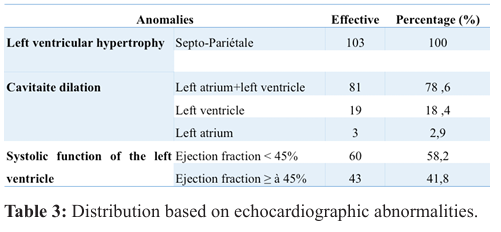
Doppler echocardiography showed an altered left ventricular ejection fraction (less than 45%) in 58.25% (Table 3) of cases and left ventricular hypertrophy in all patients with a predominance of the concentric type (52.9%).
The mean age of the population was 52 years (15-82 years) with a male predominance of 63% and a sex ratio of 1.7.
High blood pressure was previously known and irregularly followed in a large proportion of our patients (80%) with an average duration of more than 1 year.
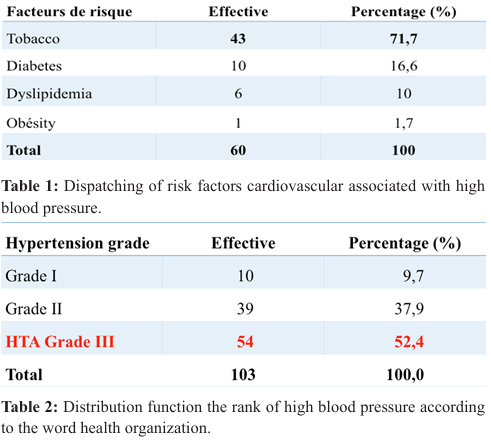
Smoking was the most common cardiovascular risk factor associated with hypertension (71.7%) (Table 1). High blood pressure grade III according to the WHO classification was found in 52.4% (Table 2). Functional signs such as dyspnea, cough and palpitations were found in 71% of cases.
Alteration of the left ventricular ejection fraction was dominant in humans with 61.1%.
Therapeutically, diuretics and conversion enzyme inhibitors were used in 73.7%, beta-blockers in 17.3% and calcium channel blockers in 9%.
Complications were dominated by congestive heart failure (52%), arrhythmia (21%) and ischemic stroke (4%). The average length of hospitalization was 8 days with extremes from 5 days to 14 days.
Survival at one year was 98.6%. The overall mortality rate was 1.97%. Lethality by gender was 3% in males with no statistically significant difference.
Comment
The hospital prevalence of hypertensive heart disease was 7.21%. This result is close to that of Lompo, which found 7.1% frequency [9]. For many authors and for our study, the frequency of hypertensive heart disease is often underestimated because of its frequent confusion with primary dilated cardiomyopathy when the history of hypertension is not known. A clear male predominance (63%) with a sex ratio of 1.7 was noted in agreement with Lompo (64.3%) [9]. It can be explained in part by the at-risk nature of the male sex in cardiovascular diseases. The age of the patients ranged from 15 to 82 years with a mean of 52 years. This result is almost comparable to that of Makalou [4] who found an average age of 57.23 years. This could be explained by the high representation of older people in the sample.
Among the modifiable factors, smoking associated with high blood pressure accounted for 71.7%. According to the literature the influence of smoking on blood pressure is difficult to specify Baer and Radichevich [10] observed an average increase in systolic blood pressure of 11 mmHg and diastolic blood pressure of 9mmHg after a cigarette in a hypertensive group; Similar results were noted in normotensive patients. This increase is believed to be related to an increase in sympathetic tone with an increased plasma norepinephrine level that lasts 15 to 20 minutes [10]. High blood pressure was previously known and irregularly followed in a large proportion of our patients (80%) with a duration of more than 1 year. This can be explained by a number of factors, including poor adherence to treatment due to drug inaccessibility, illiteracy of the population, combined with a perception of chronic disease that is only a concern when it becomes very disabling. Functional signs such as dyspnea, cough and palpitations were found in 71% of cases. This observation is in agreement with Dieudonné's (99.5%) [11]. Grade III hypertension represented 52.4%, this result is contrary to that of Dembélé. (21.5%) [12]. This difference could be explained by the high frequency of behavioural determinants of hypertension in our context. The image of cardiomegaly with 80.6% was the anomaly commonly found on facial chest radiography; this result is superimposed on that of Coulibaly who obtained 85.71% cardiomegaly; however, lower than that of Sanogo who reported 50.4% cardiomegaly [3]. The electrocardiogram showed isolated left ventricular hypertrophy in 89.3% of patients with predominance in patients with grade III hypertension with no statistically significant difference and associated with atrial fibrillation in 9.7%. This result is consistent with the data in the literature [13-16].
Doppler echocardiography showed an altered left ventricular ejection fraction (less than 45%) in 58.25% of cases and left ventricular hypertrophy in all patients with a predominance of the concentric type (52.9%). This result is lower than Diarra's which reported 93.3% [17].
Complication with congestive heart failure was the most common complication (52%). This is consistent with the data in the literature [15].
Several authors have reported that the prognosis for hypertensive heart disease in heart failure is generally poor, especially when it reaches the stage of dilated cardiomyopathy [15, 18,19]. Thus in the Framingham study, the one-year survival rates were 57% and 64% respectively for men and women.
The one-year survival of 98.6% of our patients was better than the one-year prognosis of patients in the Framingham study, where hypertensive heart disease often coexisted with coronary atherosclerosis. The overall mortality was 1.97% in our study. Lethality by gender was 3% in males with no statistically significant difference.
Conclusion
Hypertensive heart disease remains a common complication of high blood pressure. This work identified a hospital prevalence of with a clear male predominance. The major cardiovascular risk factors identified were smoking associated with hypertension. Electrocardiograms and Doppler echocardiograms remain the preferred tests not only for diagnosis but also for determining the various aspects and complications of the heart. Screening for cardiac damage is necessary in hypertensive patients to prevent or slow the progression to heart failure or even sudden death.
References
- Chobanian AV, Bakris GL, Black HR. The Seventh Report of Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; the JNC7 report. JAMA. 2003; 289: 2560-2572.
- Village O, Boudarias JP. Exploration Ultrasound Doppler of myocardiopathy Arch Mal Cœur et vx. 1996; 2: 39-45.
- Sakala KM. Complication of High Blood Pressure and their observed developments in hospital settings. Thesis Med, Bamako. 1980; 184.
- Mack D. hypertensive cardiomyopathy in the cardiac service of the Gabriel Toure hospital. Thesis Med, Bamako. 2009; 70.
- White H. Study Echocardiographic of the left ventricle's massdilatation ratio in hypertensive disease. Ann Cardiol Angéiol. 1984; 7: 459-464.
- Thiam M. Heart failure in an African cardiac environment. Bull Soc Patho Exot. 2003; 96: 217-218.
- Kama MS, kimbally KG, Gombet T, et al. Heart failure of the subject age in Brazzaville: Clinical, Etiologic and evolutionary Aspects. Med trop. 2008; 68: 60-257.
- Diallo B, Salah K, Dhar S, et al. Heart failure at the hospital Point G. Mali Med. 2004; 9: 15-17.
- Lompo Dilated cardiomyopathy at Epidemiological, clinical, paraclinical and evolutionary Aspects: about 143 cases collected from 1996 to 1999. Thesis Med, Ouagadougou. 2001; 24.
- Baer L, Radichevich I. Cigarette smoking in hypertensive patients.Blood pressure and endocrine reponses. Am J med. 1985; 78: 564-568.
- Dini GYN. Dilated cardiomyopathy in the Department of Cardiology B of the hospital of Point G. Epidemiological, clinical, and causative study. Thesis Med, Bamako. 2002; 59.
- Maxime D. The place of high blood pressure in the medium specialises cardiac of Hospital Gabriel Toure. Thesis Med, Bamako. 2011 ; 25.
- Waeber BWR, Brunner HR. Pathophysiology of left ventricular hypertrophy. Arch Mal Cœur. 1995; 88: 9-14.
- Malu K, Eboule C, Ticolat R, et al. Study of the mass/diameter ratio of the left ventricle in cardiomyopathies in black Africa (data echocardiographic, hemodynamic and Angiographic). Cardiol trop. 1990; 16: 141-148.
- Bayés GAMO, Guinda JMO, Vinolas XMO, et al. Cardiac arrhythmias and left ventricular hypertrophy in systemic hypertension and their influences on prognosis. Am J CardioI. 1995; 76: 54-59.
- Harris J, Marais N, Gay J, et al. Apparently primitive cardiac deficiencies of ischemic origin: elements of clinical diagnosis. Arch Mal Coeur. 1970; 3: 324-337.
- Diarra IM. Electrocardiographic and echocardiographic Aspects of high blood pressure about 150 cases. Thesis Med, Bamako. 2001; 29.
- Bearti B, Datta BN. Hypertension and dilated cardiomyopathy (idiopathic cardiomegaly): an autopsy experience 42 cases. Cardiol Trop. 1987; 13: 145-148.
- Anjorin FI, Okeahialam BN. Observation at echocardiography in dilated cardiomyopathy in Nigerians. Cardiol trop. 1994; 20: 127-129.