Management of Cardiovascular Emergencies in Ziguinchor: Difficulties and Prospects in Semi - Urban Areas. About a Prospective Study at the Hospital de La Paix in Ziguinchor
Author'(s): Simon Manga1*, Mohamed Leye2, Momar Dioum2, Quinta Indafa Te1, El Hadj Mbacké Sarr2, Arame Diagne2, Sidy Lamine Sy2 and Ibrahima Bara Diop2
1Cardiology Department, Ziguinchor Hospital de la Paix, Assane Seck University of Ziguinchor, Senegal, West Africa.
2Cardiology Department, Fann National Hospital, Cheikh Anta Diop University of Dakar, Senegal, West Africa.
*Correspondence:
Dr. Manga Simon, Cardiology Department of Hospital de la Paix, Ziguinchor. Assane Seck University of Ziguinchor, Senegal, Tel: +221 77 650 25 32; Fax: 33 991 68 09; E-mail: mangasimon2@gmail.com.
Received: 21 November 2018; Accepted: 07 December 2018
Citation: Simon Manga, Mohamed Leye, Momar Dioum, et al. Management of Cardiovascular Emergencies in Ziguinchor: Difficulties and Prospects in Semi-Urban Areas. About a Prospective Study at the Hospital de La Paix in Ziguinchor. Cardiol Vasc Res. 2018; 2(4): 1-4.
Abstract
Introduction: Cardiovascular diseases are one of the leading causes of death in the world. In our countries, they are underestimated because of the insufficiency of the diagnostic means. The purpose of our study was to evaluate the management of cardiovascular emergencies at hospital de la Paix in Ziguinchor, to identify problems related to the caring and to propose solutions to improve it.
Methods: We conducted a prospective 18-month study at the Emergency Department of the hospital la Paix in Ziguinchor. We included all hospitalized patients for cardiovascular emergency during the study period. The studied parameters were socio - demographic data, antecedents, field, time of consultation, means of transport, time of care, main reason for hospitalization, medical diagnosis and evolutionary modalities.
Results: The average age was 57.5 ± 15 years with female predominance (52.9%). Majority of our patients were of low socioeconomic status (53.6%). Transport mode was unsafe in the majority of cases (73.3%). Average consultation time was 10 days and the average time to take care was 2 hours and 30 minutes. Hypertension was the main cardiovascular risk factor (60.1%) and acute dyspnea, the main reason for hospitalization (56%). Cardiomyopathy was the main underlying pathology. A mortality rate of 26.8% and an average ICU length of stay of 4.32 ± 2 days were noticed.
Conclusion: Cardiovascular emergencies are common. They are dominated by hypertensive emergencies in our series, the mode of transport is inadequate, consultation time is long and mortality rate is high.
Keywords
Introduction
Cardiovascular diseases (CVD) are currently responsible for the majority of deaths worldwide and their incidence is increasing in all countries despite improved management [1].
In 2015, the number of deaths attributed to CVD was estimated at 15 million [2]. Sub- Saharan Africa is not spared from this scourge. In 2013, about 1 million deaths were attributable to CVD in Sub - Saharan Africa; which accounted for 5.5% of all CVD-related deaths globally, 11.3% of all-cause deaths and 38% of non-communicable disease related deaths [3]. This reflects the epidemiological transition marked by the gradual decline of infectious diseases and the development of chronic noncommunicable diseases. Most of these CVD occur in a lifethreatening emergency setting.
In Senegal, they account for 46% of medical emergencies [4].
The large influx of patients received in the Emergency department (ED) of the Ziguinchor Peace Hospital (South of Senegal) in a cardiac emergency situation led us to carry out this work, whose objective was to evaluate the management of cardiovascular emergencies in Ziguinchor, to identify the difficulties of management and to propose solutions to improve the management of cardiovascular emergencies in Ziguinchor.
Methodology
We conducted a prospective study over a period of 18 months (March 2017 to September 2018) at the Emergency department (ED) of the hospital de la Paix in Ziguinchor.
We included all patients admitted to the ED for cardiovascular emergency during the study period. Namely: cardio - circulatory arrest, acute pulmonary edema, cardiogenic shock, acute coronary syndromes (ACS), aortic dissections, pulmonary embolism (PE), pericarditis, severe rhythm or conduction troubles and hypertensive emergencies.
We made a record of support which included socio-demographic data, personal and family history, terrain, time of admission (delay between onset of signs and arrival at the hospital), referral system, mode of transportation, reasons for admission, time to medical care at the ED, clinical and paraclinical data, and mode of evolution.
The data were analyzed using SPSS software version 22.
Results
We included a total of 153 patients during the study period. Cardiovascular emergencies accounted for 11.7% of all hospitalizations at the ERU during the same period.
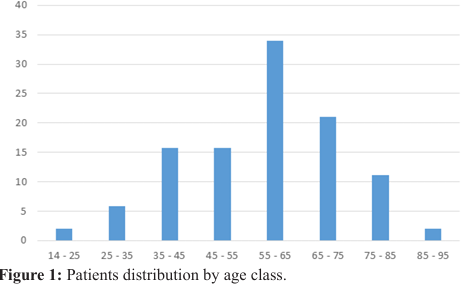
The average age of our patients was 57.5 years (range, 14 to 92 years) and the most represented age group was 55 to 65 years of age (Figure 1). Our patients were predominantly female (52.9%) with a male / female sex ratio of 0.88.
Most of our patients were of low socioeconomic status (53.6%) and most of them were not referred by a medical facility (64.5%).
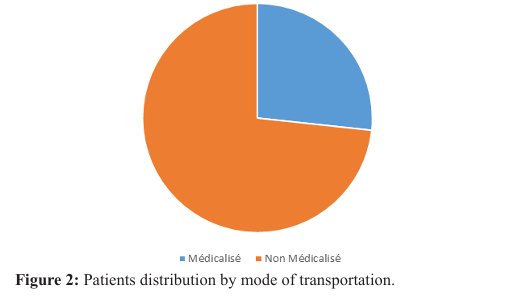
Non-medicalized mode of transport was mostly used (73,3%) (Figure 2).
An average consultation time of 10 days (range of 0.4 to 30 days) and an average cardiac management time of 2 hours 30 minutes (range of 24 minutes and 5 hours 15 minutes) were noticed.
Acute dyspnea was the main reason for emergency admission. The (Figure 3) summarizes the main reasons for admission to ED.

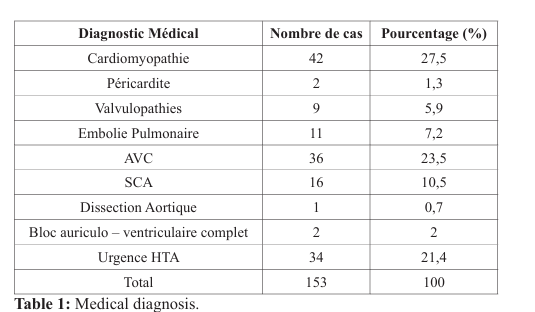
Hypertension was the main cardiovascular risk factor (60.1%) and cardiomyopathies were the main underlying pathology (Table 1).
Average duration of hospitalization : 4.32 days (range 1 to 12 days).
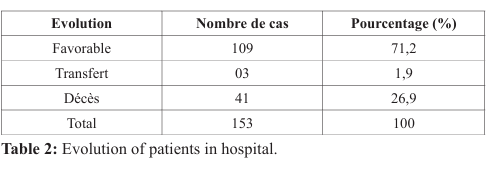
The evolution was favorable in most cases and the mortality rate was 26.8% (Table 2).
Discussion
The frequency of cardiovascular emergencies in our study was 11.7% much lower than the one of KANE [4] and MBOLOSIA [5] where they accounted respectively for 46% and 32.52% of hospitalizations. This difference is due to the versatile nature of our emergency unit which, apart from cardiovascular emergencies, also receives emergencies from other medical specialties. We do not have specialized cardiovascular emergencies support units.
Our patients were relatively young compared to those of Western series. The average age in our study was 57.5 years comparable to that of several African series [4-8] while it is 67 years in the Western series [8]. This is probably due to easier, earlier access to care and better therapeutic education.
Most of our patients are of low socioeconomic status, which can also be a barrier to early consultation.
The time between the onset of symptoms and arrival at the hospital is long. It was 10 days in our study, longer than other series where it ranged between 1 and 07 days [4,7,10]. This is certainly due to the limited means of most patients who initiated a late consultation.
The way of transport is unsafe for the most part. In our study, only 26.8% of patients arrived by ambulance while in other series, this involved an average of 5% of patients [6,9]. Our hospital is a reference structure that polarizes several health districts that are referential structures in case of emergency.
The main cardiovascular emergencies profile found in our study is comparable to the results of the other authors [4-7,10,11] and confirms the prominent place of hypertension as a major cardiovascular risk factor involved in stroke and acute heart failure. Underlying conditions were cardiomyopathies (27.5%), stroke (23.5%) and severe hypertension (21.4%). Coronary heart disease was involved in 10.5% of cases.
The mortality rate is high. It is 26.9% in our study with variable proportions depending on the series and ranging from 4% [6] to 50% [4]. This high mortality is attributable to several factors: the low socioeconomic level of our patients, the long consultation period, the unsuitable mode of transport and the insufficiency of the technical platform of our emergency services.
This work allows us to formulate several proposals to reduce morbidity and mortality related to cardiovascular diseases in an African continent in the midst of an epidemiological transition. The fight against the danger of cardiovascular diseases can not be achieved without an effective prevention policy against cardiovascular risk factors by informing and properly educating populations.
This fight also involves the establishment of mutual health to promote access to care for the poorest layers, the regional construction of cardiology centers with cardiology intensive care units meeting standards [12], quality training of caregivers in the timely and adequate management of CVUs and the regional establishment of SAMU with availability of an emergency call center to reduce consultation times and care because "time is golden" in Cardiology.
Conclusion
Cardiovascular diseases are responsible for the majority of deaths worldwide and are frequently in the form of CVE.
The practitioner, most often the cardiologist, has to deal with a variety of situations that are life-threatening in the short term.
Management of cardiovascular emergencies in Ziguinchor faces many problems. Our study shows that it concerns a young and economically active population in our regions. It also reveals long consultation times and an unsuitable mode of transportation.
It also reveals the central role of hypertension as a major cardiovascular risk factor and a high mortality.
Reducing this mortality will require an effective prevention policy against cardiovascular risk factors and good regional organization of the cardiovascular emergency management system.
References
- Mattu A, Brady WJ, Bresler MJ, et al. Cardiovascular emergencies. American College of Emergency Physician. 2015; 1-24.
- Chang YJ, Chang SL, Chong E, et al. Cardiovascular Emergencies. Biomed Research International. 2017; 1-2.
- Keates AK, Mocumbi AO, Ntsekhe M, et al. Cardiovascular disease in Africa : epidemiological profile and challenges. Nature Review Cardiology. 2017; 1-21.
- Kane A, Ndiaye A, Diao M, et al. Prise en charge des urgences cardio – vasculaires au Sénégal. Cardiol Trop. 2002; 28: 1516.
- Mboliasia I, Lepira B, Makulo R, et al. Profil épidémiologique et clinique des urgences cardiovasculaires admises aux soins intensifs de médecine interne des cliniques universitaires de Kinshasa. Ann Afr Med. 2015; 8: 1933-1938.
- Gombet T, Ellenga – Mbolla BF, Ikama MS, et al. Urgences cardio – vasculaires au centre hospitalier et universitaire de Brazzaville. Médecine d’Afrique Noire. 2007; 54: 505-511.
- Hamadou B, Kalissou YT, Jingi MA, et al. Clinical presentation and outcome of cardiovascular emergencies in Yaounde: A cross – sectional study. World Journal of Cardiovascular Diseases. 2018; 8: 133-142.
- Sarr SA, Babaka K, Archich N, et al. Profil des patients admis en unité de soins intensifs dans un service ce cardiologie de Dakar. Rev CAMES SANTE. 2017; 5: 83-87.
- Koegler A, Roul G, Bareiss B, et al. Mortalité à 4 ans de l’insuffisance cardiaque à fonction systolique conservée. Arch Mal Cœur. 1995; 88: 961-966.
- Bertrand E, Muna WE, Diouf SM, et al. Urgences cardiovasculaires en Afrique sub – saharienne. Arch Mal Cœur Vaisseaux. 2006; 99: 1159-1165.
- Hailemariam T. Prevalence of cardiovascular Emergencies in Specialized Hospital, Addis – Abeba, Ethiopia. Emergency Med. 2014; 4: 1-5.
- Beaufils P, Besse P, Charbonnier B, et al. Recommandations de la société française de cardiologie pour la prise en charge des urgences cardiologiques. Arch Mal Cœur Vaisseaux. 1999; 92: 337-345.
- Bertrand E. Evolution et état actuel des maladies cardio – vasculaires en Afrique sub – saharienne. Soc Pathol Exot. 2008; 1-5.
- Nallet O, Ketata N, Ferrier N, et al. La prise en charge rapide des douleurs thoraciques aux urgences. Ann Card Angeiol 2006; 65: 326-329.