Peripheral Arterial Disease of the Lower Limbs: Epidemiological and Ultrasound Profile of Patients with Stenosis at the Conakry University Hospital
Author'(s): Balde MD1, Bah MB1, Balde EY1, Beavogui M1, Camara A1*, Tamko C1, Barry IS1, Balde MA1, Kone A2, Sylla IS1, Diakite S3, Diallo M and Conde M1
1Cardiology Department of Ignace Deen Hospital.
2Cardiology Department of Donka Hospital.
3Cardiology Department of Camp Samory Hospital Military.
*Correspondence:
Camara Abdoulaye, Cardiology Department of Ignace Deen Hospital, 621 2266 81.
Received: 24 May 2021; Accepted: 21 June 2021
Citation: Balde MD, Bah MB, Balde EY, et al. Peripheral Arterial Disease of the Lower Limbs: Epidemiological and Ultrasound Profile of Patients with Stenosis at the Conakry University Hospital. Cardiol Vasc Res. 2021; 5(3): 1-4.
Abstract
Introduction: Peripheral arterial disease of the lower limbs (PAD) is a partial or total obliteration of one or more arteries intended for the lower limbs by atheroma. Its prevalence increases with age, but also with other major cardiovascular risk factors such as diabetes, smoking, high blood pressure and dyslipidemia. Its diagnosis is essentially based on arterial Doppler ultrasound, which studies the topography and extension of the lesions, thus constituting the essential tool for therapeutic decision-making. The objective was to describe the epidemiological and ultrasound profile of patients with atheromatous arterial stenosis of the lower limbs.
Methodology: This was a cross-sectional descriptive study running from 1 January 2019 to 31 March 2020, we took a duration of 15 months. This study was carried out at the Conakry University Hospital (Donka and Ignace Deen Hospitals).
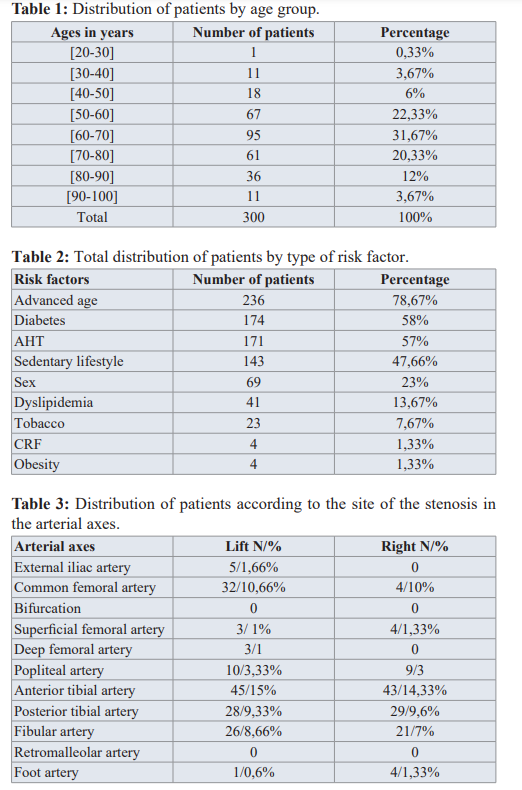
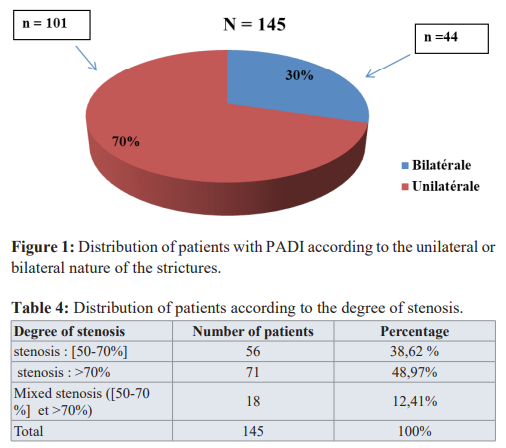
Results: In our series, the average age was 64.7 ± 13 years, with a sex ratio of 1.04. The average age was 64.7 ± 13 years, with a sex ratio of 1.04. The average age of the women in our series was 64.7 ± 13 years. Risk factors were dominated by advanced age (78.67%), diabetes (58%), hypertension (57%) and physical inactivity (47.66%). Among the 300 patients, 145 were carriers of atheromatous arterial stenosis, or a frequency of 48.33%. The leg arteries were the most affected, followed by the common femoral arteries. Concerning the degree of stenosis, patients with stenosis greater than 70% were the most represented.
Conclusion: Peripheral arterial disease of the lower limbs (AOMI) is a pathology not to be neglected in Guinea. Patients have several risk factors : stenosis is an important part of the ultrasound lesions of this disease
Keywords
Introduction
Arteriopathy obliterating of the lower extremities (PAD) is the consequence of the development of atherosclerotic lesions which gradually obstruct the lumen of the arteries and create an obstacle to the distal vascularization of the lower extremities. It is a chronic and frequent disease whose prevalence increases markedly with age [1]. However, high blood pressure, diabetes, smoking and dyslipidemia are the main risk factors for atherosclerosis, the most common etiology of peripheral arterial disease [2]. Medical imaging is essential in the exploration and even the treatment of arterial involvement. In fact, Doppler ultrasound, angio-scanner, magnetic resonance angiography and arteriography of the lower limbs make it possible to make the diagnosis of arterial disease and to predict a possible surgical or radiological revascularization of the pathological artery. . In Sub-Saharan Africa, the lack of means of the population and the absence of social security limit vascular exploration of the AOMI to doppler ultrasound which is the only available and inexpensive technique [3]. Arterial Doppler is a non-invasive, accessible and reproducible but operator dependent examination which allows a satisfactory morphological and hemodynamic analysis of the different arterial axes [4]. It is estimated that more than 200 million people are affected by this disease worldwide [5]. It reaches 6.9 to 19.1% of subjects over 40 years of age in Western countries [6]. The insufficient statistical data on PAD in our practice environment, the functional disability of patients after amputation for the most part and the lack of long-term follow-up in his atherosclerotic patients with adequate drug treatment are all reasons why motivated us to carry out this study, the objective of which was to describe the epidemiological and ultrasound profile of patients referred to vascular Doppler ultrasound for suspected atheromatous stenosis of the lower limbs.
Methodology
This is a cross-sectional, descriptive study running from January 1, 2019 to March 31, 2020, for a period of 15 months. All patients who performed arterial Doppler ultrasound in the ultrasound laboratory during this period were included in the study. We excluded from our study all the patients who presented signs in favor of an acute ischemia of the non-atheromatous lower limbs, a cyst or an aneurysm, all isolated. The cardiology department of the Ignace Deen national hospital of the Conakry CHU served as the framework for this study.
The parameters studied were as follows: Sociodemographic characteristics: age, sex Cardiovascular risk factors: smoking, hypertension, diabetes, obesity, sedentary lifestyle, dyslipidemia, CRF, advanced age, males.
Data on the ultrasound features of the stenosis:
Epidemiological
Hypertension was considered to be FDRCV in all patients declared hypertensive, treated or not. For diabetes, these were known diabetic patients who were balanced or not with or without treatment. All patients who regularly smoke cigarettes or who have been weaned less than 3 years before their inclusion in the study were selected as tobacco users. Dyslipidemia was defined according to the criteria of the National Cholesterol Education Program Adult Treatment Panel III and / or patients on lipid- lowering treatment [7]. Obesity was defined by a BMI ≥30kg / m2 and / or a waist circumference greater than 88 cm in women and 102 in men [8]. Sedentary lifestyle was defined as the absence of regular physical activity or less than 30min 3 times a week. Advanced age was considered a risk factor in all men aged 50 or over; or in all women aged 60 or over [8].
Ultrasound
Stenosis: It was a narrowing of the caliber of the arterial lumen expressed as a percentage. Stenosis assessment protocol: The diagnosis of stricture was based on the criteria of COSMANN et al. [9] as well as the hemodynamic repercussions downstream for stenoses %70%. Moderate stenosis: it was a narrowing of the caliber of the arterial lumen of between 50 and 70% Tight stenosis: it was defined by a narrowing of the caliber of the arterial lumen greater than 70%. The analysis and processing of the data were carried out by the EPI info software in version 7.2.2.6 The software from the 2010 office pack (Word, Excel, etc.) was used for entering the document, designing tables and figures. The proportions were used to describe the qualitative variables.
Results
A total of 300 patients participated in the study whose mean age was 64.7 ± 13.05 years with ranges of 28 and 96 years, the median age was 64 years. The most represented age group was between 60 and 70 years old, or 31.67%. Table I represents the total distribution of patients by age group. There was a slight male predominance 153 (51%) against 147 (49%) for women with a sex ratio of 1.04. We found an average of 2.9 ± 1.5 cardiovascular risk factors per patient whose extremes were 0 and 5 risk factors with more than half of the patients who had at least 3 risk factors. The risk factors were dominated by age (78.67%), Diabetes (58%), hypertension (57%) and physical inactivity (47.66%).
Discussion
Age is an established risk factor for the development of arteriopathy obliterans of the lower limbs. According to some studies the prevalence of PADI increases with age similarly in both sexes [10].
In our series the mean age of the study population was 64.67 years, the extreme ages of our patients were 28 and 97 years. This average age shows that obliterating arterial disease of the lower limbs is a pathology in the elderly. In some studies, PADI has been shown to preferentially affect 1.38 times more men than women [11]. We found results going in this direction with a male predominance of 51% and a sex ratio M / F of 1.04.
In our series we found an average of 2.9 ± 1.5 risk factors whose extremes were 0 and 5 risk factors with more than half of the patients having at least 3 risk factors. Our results are close to those reported by Menanga et al. during their study who had an average of 3.2 risk factors, with more than half of their patients having 3 or more risk factors [2]. Testifying to the polyfactorial association of this disease. In our series, the risk factors were dominated by advanced age (78.67%), Diabetes (58%), hypertension (57%), sedentary lifestyle (47.66%). Our results are close to those found by Merghit et al. who found advanced age as a risk factor with a frequency of 69% [12]. Diabetes is a major cardiovascular risk factor that has become epidemic in several developing countries during the last decade [1].
It was the 2nd risk factor for PAD with 58% of cases. This proportion represents around three times the data found in the general literature. This intimate relationship between diabetes and PADI has also been reported by Belaye et al. who found a frequency of diabetes of 63% [13]. In our study, although having a high proportion (57%), hypertension was not the primary risk factor for PAD as described in the literature [1]. Merghit et al. had found a frequency close to ours, ie 58.8% [12]. On the other hand, Meloni et al had found hypertension as the 1st risk factor in diabetics with a frequency of 86% [14]. These different values testify to the major role of hypertension in the occurrence of arteriopathy obliterans of the lower limbs in black African subjects. In our study, sedentary lifestyle came in 4th position with a frequency of 47.66%, in agreement with those found by Behar et al who found a proportion of 43.6% of sedentary subjects [15].
We found dyslipidemia in 13.67% of our subjects, this is close to the results found by Joosteen et al. which was 17% [16]. Tobacco intoxication was found in 7.67% of our patients. Our results are close to those found by Salimanou et al. who obtained a frequency of 5.2% of smoking [17]. In the West, smoking is ranked the number one risk factor for the PIA [1]. The very low prevalence of smoking that we have had can be explained, among other things, by the influence of the Muslim religion which prohibits the use of tobacco especially among women. We used Doppler coupled ultrasound to screen for vascular lesions in our patients. It quickly locates the areas of turbulence allowing to focus the search for significant stenosis [3]. It more easily detects lesions at high risk of progression in critical areas (iliac, femoral and tibial tripods) [3]. Arterial Doppler ultrasound of the lower limbs provides an overview of the anatomy and hemodynamics by providing a precise description of the lesions [12].
This exploration involves the entire arterial tree from the abdominal aorta to the ankle arteries; in each territory, exploration is performed on a patient at rest, in supine and systematized according to a specific protocol for each territory [12]. In our series, we had a frequency of stenosis of 48.33%. This result is close to that reported by Goeh-Akue et al. in Togo who had a 44.59% frequency of arterial stenosis [18]. As well as that found by Kouamé et al. in Ivory Coast, which reported 43.6% of arterial stenosis [3].
We had a predominance of tight stenosis at the level of the common femoral arteries with respectively 11% on the left and 9.65% on the right. This result is close to that found by Dia et al. in Senegal in 2011 who had 13.05% severe femoral artery stenosis in diabetics [4]. We obtained a predominance of stenosis at the unilateral level in 70% against 30% had bilateral involvement. Our results are similar to those of RAJONANAHARY et al. in Madagascar who had 86% of unilateral lesions and 14% of bilateral strictures [19].
Conclusion
Obliterating arterial disease of the lower limbs (PAD) is a disease that should not be overlooked in Guinea. And atheromatous stenoses occupy an important part in ultrasound lesions. Age, diabetes, high blood pressure, and physical inactivity were the most implicated risk factors. There was multi-stage stenosis but predominant in the leg arteries. It is a serious pathology, involving the vitality of the affected limb but also the vital prognosis. Hence the interest of doing the arterial Doppler ultrasound in time, which is the cornerstone of the diagnosis.
References
- Konin C, Soya E, Koffi J, et al. Obliterating arterial disease of the lower limbs in Ivory Coast: epidemiological, clinical and quality of life aspects. Annals of Cardiology and Angiology. 2015; 67: 10.
- Menanga A, Hamadou B, Ahinaga AJ, et al. Asymptomatic arteriopathy obliterans of the lower limbs in a group of patients with cardiovascular risk factors in Yaoundé. Health Sciences And Diseases. 2014; 15: 1-7.
- Kouamé N, Koffi D, N’goan-Domoua AM, et al. Doppler ultrasound in the prevention of lower limb amputations in diabetics in Côte d'Ivoire. Nuclear medicine. 2011; 35: 533-536.
- Dia AA, Affangla DA, Dione JM, et al. Contribution of arterial Doppler ultrasound of the lower limbs in the treatment of diabetic foot at Saint-Jean de Dieu Hospital in Thies (Senegal). Pan Afr Med J. 2015; 22: 1-10.
- D’Abate F, Ramachandran V, Young MA, et al. B-flow imaging in lower limb peripheral arterial disease and bypass graft ultrasonography. Ultrasound in medicine and biology. 2016; 42: 2345-2351.
- Houenassi DM, Houehanou C, Tchabi Y, et al. Epidemiology of chronic obliterating arterial disease of the lower limbs in patients with arterial hypertension at the Cotonou University Hospital. Tropical Cardiology. 2012; 135: 1-12.
- Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome. 2005; 285-290.
- Attias D, Lellouche N. ikB Vascular cardiology. 7th edition, Vernazobres-Grego. Paris. 2015. 686.
- Cossman DV, Ellison JE, Wagner WH, et al. Comparison of contrast arteriography to arterial mapping with color-flow duplex imaging in the lower extremity. Journal of vascular surgery. 1989; 10: 522-529.
- Alessandra BR, Romain M. Obliterating arteriopathy of the lower limbs in women. Journal the medical press. 2018; 47: 62-65.
- Awalou MD, Edem KM, Agbeko KD, et al. Diabetic foot: epidemiological, diagnostic, therapeutic and evolutionary aspects at the Medical-Surgical Clinic of the Sylvanus Olympio CHU in Lomé. Pan African Medical Journal. 2018; 30: 1-5.
- Merghit R, Ait Athmane M, Lakehal A. Extracoronary atherosclerotic involvement in coronary artery disease: result of a monocentre cross-sectional study in eastern Algeria. Annals of Cardiology and Angiology. 2019; 201-206.
- Bélaye L, Lurel D, Ezelin F, et al. Obliterating arteriopathy of the lower limbs of atheromatous origin in Guadeloupe: about 268 patients. Journal of Vascular Diseases. 2016; 41: 246-252.
- Meloni M, Izzo V, Giurato L, et al. Below-the-ankle arterial disease severely impairs the outcomes of diabetic patients with ischemic foot ulcers. Diabetes research and clinical practice. 2019; 152: 9-15.
- Behar T, Bosson JL, Galanaud JP, et al. Assessment of the prevalence and risk factors of arteriopathy obliterans of the lower limbs as part of an outpatient screening campaign. Journal of Vascular Diseases. 2013; 38: 22-28.
- Joosten MM, Pai JK, Bertoia ML, et al. Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men. Jama. 2012; 308: 1660-1667.
- Amidou SA, Houehanou YC, Houinato SD, et al. Epidemiology of lower extremity artery disease in a rural setting in Benin, West Africa: The TAHES study. International journal of cardiology. 2018; 267: 198-201.
- Goeh-Akue E, Pio M, Afassinou Y, et al. Contribution of vascular doppler echo in the lesion diagnosis of open diabetic foot in type 2 diabetic in Lomé. Annals of Angelology. 2015; 67: 39.
- Rajaonanahary T, Raherinantenaina F, Rakotonaivo M, et al. Obliterating arterial disease of the lower limbs at the University Hospital of Antananarivo (Madagascar). Tropical Medicine and Health. 2014; 24: 189-193.