Sexual Dysfunction In Cirrhosis: A Prospective Multicenter Study
Author'(s): Mamadou Ngoné Gueye1*, Melissa C. E. Sengue2,3, Salamata Diallo4, Djimby Sow2, Marème Polèle Fall4, Cheikh Ahmadou Bamba Cissé1, Gnagna Diouf1, Mame Aissé Thioubou5, Mame Coumba Cissé2, Marie Louise Evra2, Marie Louise Bassène4, Daouda Dia1, and Mouhamadou Mbengue1
1Hepato-Gastroenterology Department of General Idrissa Pouye Hospital, Dakar, Senegal.
2Hepato-Gastroenterology Department of Abass Ndao Hospital, Dakar, Senegal.
3Hepato-Gastroenterology Department of the Saint-Quentin Hospital, France.
4Hepato-Gastroenterology Department of Aristide Le Dantec Hospital, Dakar, Senegal.
5Hepato-Gastroenterology Department of Peace Hospital, Ziguinchor, Senegal.
*Correspondence:
Mamadou Ngoné Gueye, Hepato-Gastroenterology Department of General Idrissa Pouye Hospital, Dakar, Senegal.
Received: 20 Feb 2022 Accepted: 23 Mar 2022 Published: 28 Mar 2022
Citation: Gueye MN, Sengue MCE, Diallo S, et al. Sexual Dysfunction In Cirrhosis: A Prospective Multicenter Study. Gastroint Hepatol Dig Dis. 2022; 5(1): 1-5.
Abstract
Introduction: All the manifestations of cirrhosis, sexual dysfunction, mainly because of its taboo nature. The least sought after by hepatologists and the least reported spontaneously by patients. Taking this condition into account is a necessity to improve the quality of life of patients.
Methods: We conducted a prospective descriptive and analytical study over 14 months from March 2020 to April 2021 in patients followed for cirrhosis. Recruitment was multicenter. We included all cirrhotic patients who gave their consent to participate in the study. The diagnosis of cirrhosis was made on the basis of clinical, biological, radiological, endoscopic and histological evidence. The classification used was the simplified ASEX classification. Each element of the classification was scored from 1 to 3. Sexual Dysfunction was defined by a total ≥7, or a score of 3 on any item, or 2 on at least 3 items. Data were entered with Sphinx software version 5.1.0.2 and analyzed with version 18. The comparison of frequencies was done using Pearson's Chi-square test or Fisher's two-tailed exact test according to their applicability conditions with a significance threshold of 0.05.
Results: We interviewed 50 patients with cirrhosis during our study period. Sexual dysfunction was observed in 34 patients, 68% of our population. The mean age was 52 years with extremes of 23 and 73 years. An age below 50 years was found in 40% of the patients.In patients with sexual dysfunction, the average age was 53 years with extremes of 35 and 73 years. Of these, 32.4% were younger than 50 years of age. The population was composed of 35 men and 15 women, for a sex ratio of 2.33. Sexual dysfunction was found in 24 men (84%). Active smoking was present in 18 patients. Alcohol abuse was present in 21 patients. Alcohol abuse was present in 21 patients. 95.2% of them had an alcohol abuse (p = 0.0001). Cirrhosis was most often associated with diabetes (13 cases), metabolic syndrome (11 cases) and hypertension (10 cases). In multivariate analysis, only diabetes was significantly associated with sexual dysfonction (p = 0.027). The most common etiologies of cirrhosis were alcohol (25 cases), HBV (15 cases), and NASH (10 cases). Sexual dysfonction was found in 84% of patients with alcoholic cirrhosis, in 80% of patients with postNASH cirrhosis, and 40% of patients with post-HBV cirrhosis. In multivariate analysis, there was a significant association between alcohol and sexual dysfonction (p = 0.015), and between HBV and Sexual dysfonction (p = 0.002). Twenty-nine patients had cirrhosis classified as CHILD A (58% of cases), and 18 patients (36% of cases) had cirrhosis classified as CHILD B. All patients with cirrhosis classified as CHILD C had sexual dysfonction. Sexual dysfonction was significantly related to the severity of the CHILD PUGH score (p = 0.002). Twenty-nine patients had cirrhosis classified as CHILD A (58% of cases), and 18 patients (36% of cases) had cirrhosis classified as CHILD B. All patients with cirrhosis classified as CHILD C had sexual dysfonction. Sexual dysfonction was significantly related to the severity of the CHILD PUGH score (p = 0.002).
Conclusion: Our study shows that about three quarters of cirrhotic patients present a sexual dysfunction. The alcoholic etiology and the severity of cirrhosis seem to be the factors associated with sexual dysfunction in cirrhotic patients.
Keywords
Introduction
Holistic management of the patient is a challenge for the practitioner when following a chronic disease such as cirrhosis. It is imperative in these patients to look for elements that may alter their quality of life, among which sexual dysfunction of all the manifestations of cirrhosis, sexual dysfunction is the least sought after by hepatologists and the least reported spontaneously by patients, mainly because of its taboo nature. Taking this condition into account is a necessity to improve the quality of life of patients. It is in this context that we decided to carry out this study whose objectives were to evaluate the frequency of sexual dysfonction in cirrhotic patients and to highlight the factors influencing the presence of sexual dysfonction in cirrhotic patients.
Patients and Methods
We conducted a prospective descriptive and analytical study over 14 months from March 2020 to April 2021 in patients followed for cirrhosis.
The recruitment was multicentric and took place in the Hepato Gastroenterology and Internal Medicine departments of 3 hospitals. The Hepato-Gastroenterology Department of the Saint-Quentin Hospital (France). The Hepato-Gastroenterology Department of the Abass Ndao Hospital (Senegal), and the Hepato-Gastroenterology and Internal Medicine Department of the Idrissa POUYE General Hospital (Senegal). The study population was composed of all patients received in consultation or in hospitalization in these different services. We included all cirrhotic patients who gave their agreement to participate in the study. The diagnosis of cirrhosis was made on the basis of clinical, biological, radiological, endoscopic and histological evidence.
Patients with atleast one of the following were not included.
- Absence of sexual activity
- Profound alteration of general condition classified as 3 to 4 according to the World Health Organization (WHO) classification;
- The presence of clinical hepatic encephalopathy;
- The lack of paraclinical information preventing the staging of cirrhotic disease;
- The existence of HCC or other associated neoplastic pathology.
All included patients were informed of the purpose of the study and gave verbal consent. Information was collected by the medical staff in strict compliance with medical confidentiality.
Patients were recruited during hospitalization and consultations. Patients who met the inclusion criteria answered the questions on a pre-established questionnaire. For illiterate patients, the questionnaire was filled out by a physician based on oral responses provided by the patient. Medical information was collected from the medical record with the agreement of the treating physician.
The classification used was the simplified ASEX classification. Each item in the classification was scored from 1 to 3. Sexual Dysfunction was defined by a total ≥ 7, or a score of 3 on any item, or 2 on at least 3 items.
Data were collected on a predesigned form. They were entered with Sphinx software version 5.1.0.2 and analyzed with SPSS (Statistical package for Social Sciences) software version 18. The comparison of the frequencies was done using the Pearson Chi- square test or the Fisher's two-tailed exact test according to their applicability conditions with a significance threshold of 0.05.
During the study, we were confronted with some difficulties. Due to the intimate nature of the subject of our study, several patients refused to participate;
The translation of the questions into local languages often made the questioning difficult;
Results
We interviewed 50 patients with cirrhosis during our study period. This population was composed of 27 patients (54%) recruited at the Saint-Quentin Hospital (CHSQ), 18 patients (36%) recruited at the Abass Ndao Hospital (CHAN) and 5 patients (10%) recruited at the General Hospital Idrissa Pouye (HOGIP).
Sexual dysfunction was observed in 34 patients, 68% of our population. The prevalence of sexual dysfunction was 52.2% in CHAN and HOGIP patients and 81.5% in CHSQ patients. The prevalence in the male population was 68.6% and 66.6% in the female population for all centers combined. The mean age was 52 years with extremes of 23 and 73 years. An age below 50 years was found in 40% of the patients. Among patients with sexual dysfunction, the average age was 53 years with extremes of 35 and 73 years of these, 32.4% were younger than 50 years of age (Figure 1).
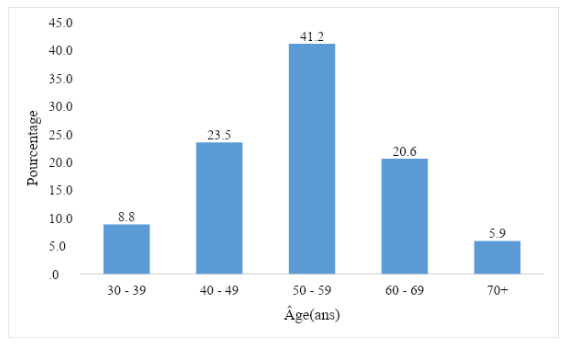
Figure 1: Distribution of Patients with Sexual dysfunction by age groups.
The population consisted of 35 men and 15 women, for a sex ratio of 2.33. Sexual dysfunction was found in 24 men (84%). Active smoking was present in 18 patients. Alcohol abuse was present in 21 patients. Alcohol abuse was present in 21 patients. 95.2% of them had an alcohol abuse (p = 0.0001). Cirrhosis was most often associated with diabetes (13 cases), metabolic syndrome (11 cases) and hypertension (10 cases) (Figure 2).
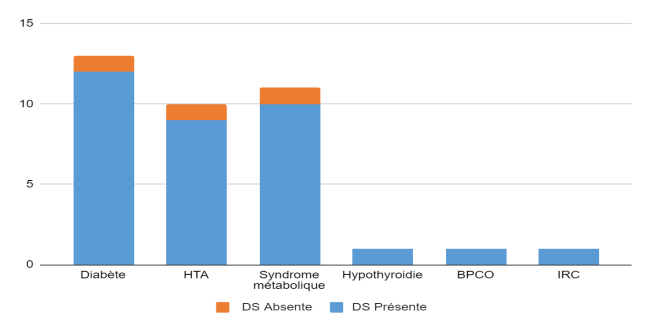
Figure 2: Distribution of Patients with Comorbidities Associated or not with Sexual dysfunction.
Sexual dysfonction was found in 92.3% of diabetic patients, in 90% of hypertensive patients, and in 90.9% of patients with metabolic syndrome.
In multivariate analysis, only diabetes was significantly associated with sexual dysfonction (p = 0.027).
The metabolic syndrome-diabetes-HTA association was present in 5 patients. All of these patients had sexual dysfonction. Medication was noted in 39 patients (78% of cases). The most frequently taken drugs were propranolol, Furosemide and Spironolactone.
Sexual dysfonction was present in 74.1% of patients on diuretics (p = 0.4) and in 66.7% of patients on Beta blockers (p = 0.603).
There was no significant association between sexual dysfonction and the different drug intakes regardless of the duration of treatment. The most common etiologies of cirrhosis were alcohol (25 cases), HBV (15 cases), and NASH (10 cases). No etiology was found in 6 patients. Several causes were sometimes incriminated in the same patient (Figure 3).

Figure 3: Distribution of Patients According to Etiologies.
Alcohol consumption was persistent in 76% of patients with alcoholic cirrhosis. The majority of patients (92%) with alcohol- related cirrhosis were recruited at CHSQ. Sexual dysfonction was found in 84% of patients with alcoholic cirrhosis, in 80% of patients with post-NASH cirrhosis and in 40% of patients with post-HBV cirrhosis in multivariate analysis, there was a significant association between alcohol and sexual dysfonction (p = 0.015), and between HBV and sexual dysfonction (p = 0.002).
Twenty-nine patients had cirrhosis classified as CHILD A (58% of cases), and 18 patients (36% of cases) had cirrhosis classified as CHILD B. All patients with cirrhosis classified as CHILD C had sexual dysfonction (Figure 4).
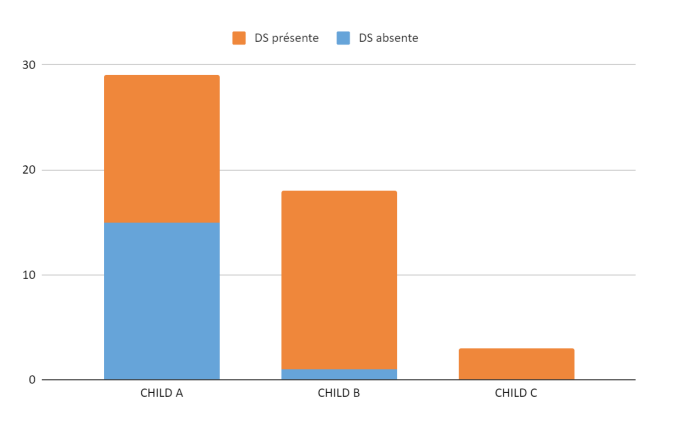
Figure 4: Distribution of Patients According to Sexual dysfunction and
CHILD PUGH score.
Sexual dysfonction was significantly related to the severity of the CHILD PUGH score (p = 0.002).
Discussion
The average age of the cirrhotic patients was 52 years with extremes of 23 and 73 years. An age below 50 years was observed in 40% of them. The average age was 52 years in France and 45 years in Senegal.
The average age in Senegal was comparable to the data found in studies in sub-Saharan Africa Indeed, Dia et al. in Senegal reported an average age of cirrhotic patients of 44.5 years [1]. Also in Senegal, Gueye et al. found an average age of 41 years [2]. In European studies, higher average ages were found, similar to the age found in our study in France [3,4].
This difference in age between European and sub-Saharan African countries is explained by the predominance of viral etiologies in sub-Saharan Africa. Since infection is generally acquired in childhood, the development of cirrhosis occurs earlier [5]. In contrast, in Western countries, daily alcohol intoxication begins in adulthood. In France, it affects 56% of men between 65 and 75 years of age, compared with 5% of men between 20 and 25 years of age [3].
A male predominance was observed in our study with a sex ratio of 2.33. This predominance was reported in numerous studies in the literature with sex ratios varying from 1.27 to 5.64 [1,6,7].
Indeed, there is a difference according to sex in the natural history of HBV, the leading cause of cirrhosis in sub-Saharan Africa. Studies have shown that in men, the evolution of liver disease is more rapid towards complications [8]. Concerning the alcoholic etiology, male consumption is more important and more frequent [9].
In our series, 58% of the patients had cirrhosis classified as CHILD A and 36% had cirrhosis classified as CHILD B.
Among the patients recruited at CHSQ (France), 48.1% had CHILD A cirrhosis. The same percentage of CHILD B cirrhosis was found. In 3.8% of patients, CHILD C cirrhosis was found at CHAN and HOGIP (Senegal), CHILD A, B and C cirrhosis were found in 69.6%, 21.7% and 8.7% of patients respectively. Analysis of several African studies shows a higher Child score (B or C) in sub-Saharan African patients [10,11].
This is probably due to the fact that in developing countries, delay in consultation is frequent due to poverty and illiteracy. Thus, patients are most often managed after the occurrence of decompensation. The results of our study show a different trend. Indeed, most of the patients with a CHILD PUGH C score were not included in our study because they presented a significant alteration of the general state.
An overall prevalence of sexual dysfonction of 68% was found in our study. In sub-Saharan Africa, we did not find any study on sexual dysfunction in cirrhotic patients of both sexes.
Nevertheless, Diao et al. in 2007 [12] in Senegal found a prevalence of erectile dysfunction of 26% in patients at Aristide le Dantec Hospital. This result is significantly lower than the prevalence of sexual dysfunction reported by our study. This difference is explained by the fact that this study was conducted in the general population, in patients of whom less than 30% had underlying pathologies. In contrast, our study involved cirrhotic patients with sometimes associated comorbidities. Moreover, since erectile dysfunction is only one of the symptoms of sexual dysfunction in men, it may be absent despite the presence of sexual dysfunction [13].
In Egypt, El Atrebi et al. [14] found a prevalence of sexual dysfunction of 29.4% in men. The fact that this frequency is very low compared to ours can be explained by the fact that only cirrhosis of viral C etiology (HCV) was taken into account in this study.
In the West, prevalences similar to ours have been reported. In Denmark, Jensen et al. found a prevalence of sexual dysfunction of 61% in patients with alcoholic cirrhosis [15]. Similarly, in the United States, Steel et al. [16] found a prevalence of sexual dysfunction of 71% in cirrhotic men of all etiologies.
We note from these figures that the prevalence of sexual dysfunction in cirrhotic patients is generally greater than 60%. The average age of patients with sexual dysfonction was 53 years of these, 32.4% were younger than 50 years. A difference in the prevalence of sexual dysfunction was noted in our study between patients incused in France and those included in Senegal with respectively 52.2% and 81.5% of sexual dysfunction in patients recruited in Senegal (CHAN and HOGIP) and patients recruited in France (CHSQ). This can be explained by the predominance of alcoholic etiology in France, but also by the fact that the CHSQ patients were older overall, with an average age of 52 years compared to 45 years in Senegal.
We found a strong correlation between tobacco consumption and sexual dysfonction. Moreover, diabetes was the only comorbidity for which a significant association with sexual dysfonction was found. Several authors report results similar to ours. Paternostro et al. [62], Huygues et al. [36] found a significant association between ED and diabetes and smoking. The comorbidities that have also been reported are cardiovascular disease and depressive syndromes [17,18].
Overall, these results are not surprising, as the effects of metabolic syndrome on sexual function have been repeatedly described in the literature, mainly through the production of inflammatory cytokines and alteration of endothelial cells [19,20].
Drug use was found in 78% of our patients. Sexual dysfonction was present in 74.1% of patients on diuretics and in 66.7% of patients on beta blockers. Our results are in agreement with those of some authors such as Maimone et al. [21] who found no significant relationship between sexual dysfonction and the use of drugs (diuretics, beta blockers, statins, antidiabetics and proton pump inhibitors). Sexual dysfonction was found in 84% of patients with alcoholic cirrhosis, in 80% of patients with post-NASH cirrhosis and in 40% of patients with post-HBV cirrhosis. Harmful alcohol use was continued in 76% of patients with alcoholic cirrhosis.
In multivariate analysis, there was a significant association between sexual dysfonction and alcoholic cirrhosis (p = 0.015) as well as viral B cirrhosis (p = 0 .002). HBV was inversely related to the risk of developing sexual dysfonction. These results are comparable to those of Huyghes et al. who identified alcohol as a risk factor for sexual dysfonction in cirrhotic patients [17]. Similarly, Kadiyala et al. found an influence of alcohol on sexual dysfonction [22].
No clear pathophysiological mechanism has been demonstrated between ED and viral hepatitis. However, there are several studies that have shown a more pronounced hypogonadism in patients with alcoholic cirrhosis, which explains the ED in these patients [23-25].
Half of the patients with sexual dysfonction had CHILD B stage cirrhosis (50%). All patients with cirrhosis classified as CHILD C had sexual dysfonction. Sexual dysfonction was significantly related to the CHILD PUGH score (p = 0.002).
In Nigeria, Adekanle et al. found more signs of sexual dysfonction in CHILD B and C patients [10]. Similarly, Gentile et al. in Italy identified the stage of cirrhosis as an independent factor for the occurrence of sexual dysfonction [26]. The South Korean team of Kim et al. identified serum albumin level as an independent factor for sexual dysfonction [27]. This may be explained by the role of albumin in testosterone transport [20].
Conclusion
Improving quality of life is a major objective in the management of cirrhotic patients. Sexual disorders, which are very frequent in this field, are often underestimated by practitioners, although their frequency seems to be very high. Our study shows that about three quarters of cirrhotic patients have sexual dysfunction. The alcoholic etiology and the severity of cirrhosis seem to be the factors associated with sexual dysfunction in cirrhotic patients.
References
- DIA D, Diouf G, Gueye MN, et al. Clinical, paraclinical and etiological aspects of cirrhosis in a department of internal Medicine in Senegal. Adv Res Gastroenterol Hepatol. 2019; 12: 49-51.
- Guèye MN, Bassene ML, Diallo S, et Electrocardiographic and echocardiographic abnormalities during viral cirrhosis B: about 60 cases in the hepato-gastroenterology department of the Aristide Le Dantec hospital in Dakar (HALD). Pan Afr Med J. 2018; 25: 169-175.
- Buscail C, Bourcier V, Fezeu L, eta l. Dietary behaviors of patients with compensated and uncomplicated cirrhosis: a case-control study in the Ile-de-France region. Nutr Clin et Métab. 2018; 32: 337-338.
- D'amico G, Pasta L, Morabito A, et al. Competing risks and prognostic stages of cirrhosis: a 25-year inception cohort study of 494 Aliment Pharmacol Ther. 2014; 39:1180-1193.
- World Health Organization. Guidelines for prevention, care, and treatment of persons with chronic hepatitis B infection. 2015; 10-2.
- Diarra M, Konaté A, Soukho AK, et al. Evolutionary aspects of cirrhotic disease in a hepato gastroenterology service in Mali. Mali Med. 2010; 25: 42-46.
- Doffou AS, Bangoura AD, Kouame GD, et al. Alcoholic cirrhosis in black Africans at the University Hospital of Yopougon: epidemiological, clinicaland biological characteristics. Rev Int Sc Med Abj. 2019; 21: 212-218.
- Chu CM, Liaw YF, Sheen IS, et al. Sex difference in chronic hepatitis B virus infection: an appraisal based on the status of hepatitis B antigen and antibody. Hepatology. 1983; 3: 947-950.
- Canarelli T, Cadet-Tairou A, Palle C. Indicators of alcohol- related morbidity and mortality in France. Bull Epidemiol Hebdo. 2006; 34: 252-255.
- Adekanle O, Ndububa DA, Orji EO, et al. Assessment of the sexual functions of males with chronic liver disease in South West Nigeria. Ann Afr Med. 2014; 13: 81-86.
- Duah A, Nkrumah KN, Tachi K. Oesophageal varices in patients with liver cirrhosis attending a major tertiary hospital in Ghana. Pan Afr Med J. 2018; 31: 230-239.
- Diao B, Ndoye AK, Fall PA, et al. Erectile dysfunction in Senegal: epidemiological profile. 2007; 17: 223-229.
- Rudler M, Bouzbib Sexual dysfunction and cirrhosis. Hepato gastroenterologist letter. 2020; 23: 124-158.
- El-Atrebi KA, El-Atrebi MA, El-Bassyouni HT. Sexual dysfunction in males with hepatitis C virus: relevance to histopathologic changes and peginterferon treatment. Saudi J Gastroenterol. 2011; 17: 406-410.
- Jensen SB, Gluud C. Copenhagen Study Group for Liver Diseases. Sexual dysfunction in men with alcoholic liver cirrhosis. A comparative study. Liver. 1985; 5: 94-100.
- Steel J, Hess SA, Tunke L, et Sexual functioning in patients with hepatocellular carcinoma. Cancer. 2005; 15: 2234-2243.
- Huyghe E, Kamar N, Wagner F, et Erectile dysfunction in end-stage liver disease men. J Sex Med. 2009; 6: 1395-1401.
- Paternostro R, Heinisch BB, Reiberger T, et al. Erectile dysfunction in cirrhosis is impacted by liver dysfunction, portal hypertension, diabetes and arterial hypertension. Liver Int. 2018; 38: 1427-1436.
- Hawksworth D, Burnett L. Nonalcoholic fatty liver disease, male sexual dysfunction, and infertility: common links, common problems. Sex Med Rev. 2020; 8: 274-285.
- Neong SF, Billington EO, Congly Sexual dysfunction and sex hormone abnormalities in patients with cirrhosis: review of pathogenesis and management. Hepatology. 2019; 69: 2683-2695.
- Maimone S, Saffioti F, Oliva G, et al. Erectile dysfunction in compensated liver Dig Liver Dis. 2019; 51: 843-849.
- Kadiyala PK. Sexual dysfunction assessed by IIEF in men with alcohol dependence - A case-control Int J Psychol. 2019; 11: 40-45.
- Coelho JC, Matias JE, Pissaia JA, et Sexual dysfunction in males with end-stage liver disease: partial recovery after liver transplantation. J Liver Dis Transplant. 2014; 3: 632-638.
- Martínez-Riera A, Santolaria-Fernández F, Gonzalez Reimers E, et al. Alcoholic hypogonadism: hormonal response to clomiphene. Alcohol. 1995; 12: 581-587.
- Neong SF, Billington EO, Congly Sexual dysfunction and sex hormone abnormalities in patients with cirrhosis: review of pathogenesis and management. Hepatology. 2019; 69: 2683-2695.
- Gentile I, Fusco F, Buonomo AR, et al. Prevalence and risk factors of erectile dysfunction in patients with hepatitis B virus or hepatitis C virus or chronic liver disease: results from a prospective study. Sex Health. 2018; 15: 408-412.
- Kim M, Kim SY, Rou WS, et al. Erectile dysfunction in patients with liver disease related to chronic hepatitis B.Clin Mol Hepatol. 2015; 21: 352-357.