Study on The Nosological Groups of Hospitalized Patients in The Cardiology Unit of Hospital Principal De Dakar in Senegal in June 2018
Author(s): Mingou JS1*, Ka M1, Sangaré Z2, Archich N2, Ndao SCT1, Dia K1, Mboup MC1 and Fall PD1
1Department of Cardiology, Hospital Principal, Dakar, Senegal.
2Department of Cardiology, Hospital Aristide Le Dantec, Dakar, Senegal.
*Correspondence:
Mingou JS, Department of Cardiology, Hospital Principal, Dakar, Senegal.
Received: 01 August 2019; Accepted: 19 August 2019
Citation: Mingou JS, Ka M, Sangaré Z, et al. Study on The Nosological Groups of Hospitalized Patients in The Cardiology Unit of Hospital Principal De Dakar in Senegal in June 2018. Cardiol Vasc Res. 2019; 3(4); 1-3.
Abstract
Introduction: Cardiovascular disease is the leading cause of death in the world. The knowledge of the prevalence of risk factors in our contexts gives an insight into the frequency of certain pathologies. The knowledge of the nosological frameworks in a hospital structure is relevant for the orientation of the objectives of raising the technical plateau to ensure optimal care.
Objective: The general objective was to study the nosological frameworks of patients hospitalized in the cardiology department of Hospital Principal of Dakar (HPD) in Senegal.
Patients and Methods: this was a descriptive study of patients hospitalized for cardiovascular disease in the period from June 1st to June 30th, 2018. The studied parameters concerned the epidemiological, clinical, paraclinical, therapeutic and evolutionary data.
Results: A total of 41 patients were included. The male gender predominated with a sex ratio of 2.2. The average age was 66.5 years (range: 38 to 84 years). Fourteen patients were admitted for heart failure (34%), eight for ischemic heart disease (20%), seven strokes (17%).
Cardiovascular risk factors were dominated by high blood pressure (71%), followed by lack of regular physical activity (56%) and diabetes (31%). Symptoms were dominated by dyspnea (41%), followed by chest pain (27%) and then lower extremity edema (22%). The electrocardiogram recorded atrioventricular block in 4.9% of cases, ST segment elevation in 12.2% of cases and necrosis in 7.3% of cases. Echocardiography noted a left ventricular ejection fraction of less than 30% in 10% of cases. The coronarography was performed in 5 patients (12%) and showed significant legions in two of them.
The brain scan only in patients admitted for hemiplegia and / or aphasia (7 patients) showed a stroke in all cases. Therapeutically, anticoagulants were the most prescribed (70%), followed by betablockers (56%) and statins (54%). A pace maker was implanted in 3 patients. The average duration of hospitalization was 8.6 days (4-30 days). Intra-hospital mortality was 5%. In bivariate analysis, the heart rate> 100 beats / min was a significant poor prognostic factor with a value of p = 0.019.
Conclusion: Cardiovascular diseases are more and more frequent with male predominance. The length of hospital stay and the mortality rate remain high. Therefore, an improvement in the management of these cardiovascular diseases is needed and passes primarily through the control of modifiable cardiovascular risk factors and the development of the technical plateau.
Keywords
Introduction
Cardiovascular disease is the leading cause of death in the world, causing more deaths than any other cause of death [1].
It is estimated that in 2012, 17.5 million people died of cardiac causes, representing 30% of all deaths worldwide. It is estimated that 7.5 million of these deaths are due to ischemic heart disease and 6.7 million are due to stroke [2].
Low- and middle-income countries are disproportionately affected, accounting for more than 80 per cent of deaths from cardiovascular disease, involving almost equally men and women. By 2030, nearly 23.6 million people will die of cardiovascular disease, mainly heart disease and stroke. These conditions are projected to remain the leading cause of death [2].
In cardiology, pathologies have most often the same contributing factors called cardiovascular risk factors. Some of this factors are more incriminated in the occurrence of a specific event. Thus arterial hypertension is mostly correlated with the occurrence of stroke. The knowledge of the prevalence of these risk factors in our contexts gives an insight into the frequency of certain pathologies.
The knowledge of the nosological frameworks in a hospital structure is very relevant for the enhancement of the technical platform pledge therefor an optimal support in the shortest time performance criterion.
The main objective of the study was to study the nosological frameworks of hospitalized patients in the cardiology department of the Hopital Principal of Dakar, Senegal.
Similarly, we have described the epidemiological, clinical and paraclinical aspects of the different entities and analyzed the evolutionary aspects.
This was a descriptive study over a period of one (01) month from June 1 to 30, 2018, conducted in the cardiology department of HPD. Patients hospitalized for cardiovascular disease during the study period were included. We collected the data using a counting sheet, the hospitalization register.
The studied parameters concerned the epidemiological, clinical, paraclinical, therapeutic and evolutionary data. SPSS software version 16.0 was used. The threshold of significance was retained for a value of p <0.05. The patients signed an informed consent form for the exploitation of the data.
Results
A total of 41 patients were included during the study period. Mean age was 66.5 years (range: 38 to 84 years). Male gender predominated with a sex ratio of 2.2.
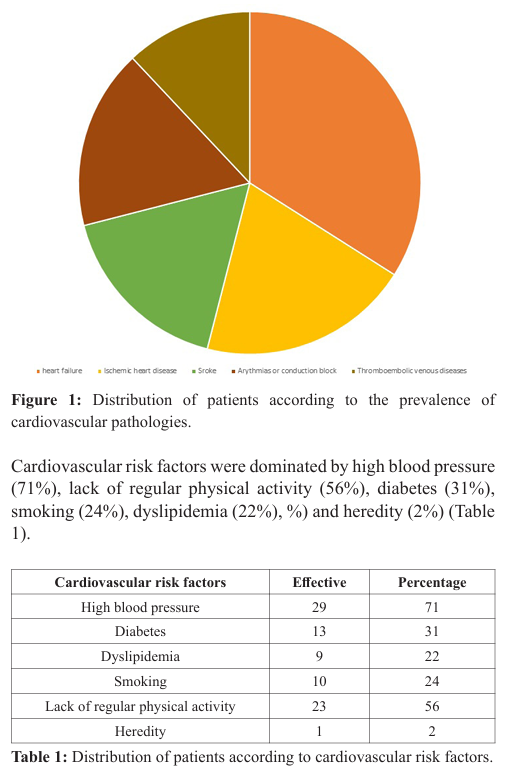
Among them 14 were admitted for heart failure (34%), eight had ischemic heart disease (20%), seven had a stroke (17%), seven had arrythmias or conduction block (17%) and 5 thromboembolic venous diseases (12%) (Figure 1).
Symptoms were dominated by dyspnea (41%) followed by chest pain (27%), lower limbs edema (22%) and palpitations (2%). Tachycardia was found in 32% of patients. The chest X-ray noted cardiomegaly in 14.6% of cases and acute pulmonary edema in 2.4% of cases. Electrocardiogram recorded atrioventricular block in 4.9% of cases, ST segment elevation in 12.2% of cases and necrosis in 7.3% of cases.
Echocardiography showed left ventricular ejection fraction of less than 30% in 10% of cases and between 30 and 50% in 30% of cases. The coronarography was performed in 5 patients (12%) and showed significant legions in two of them. Head CT was only run in patients admitted for hemiplegia and / or aphasia (07 patients) and showed a stroke in all cases.
Therapeutically, anticoagulants were the most prescribed (70%), followed by betablockers (56%), statins (54%), blockers of the renin-angiotensin-aldosterone system (inhibitors of the conversion enzyme, angiotensin II receptor antagonists) in 51% of patients, antiplatelet agents (49%), diuretics (46%) and calcium channel blockers (27%).
A pacemaker has been implanted in three (03) patients. The mean hospitalization stay length was 8.6 days (4-30 days). Intra-hospital mortality was 5%. In bivariate analysis, the heart rate> 100 beats / min was a significant poor prognostic factor with a value of p = 0.019.
Discussion
The incidence of heart failure was 34% compared to 21.6% in the pilot study in Côte d'Ivoire 2015 [3]. The incidence of ischemic heart disease was 20% of patients. This is particularly important in our population because of the particularly advanced epidemiological transition in the service, compared to a study conducted in Senegal and in the pilot study which reported respectively 9.49% and 14.7% [3].
The mean age of our population is quite high (65.5 years) compared to the Ivory Coast where it was 51 years old [3]. The predominance was male; this again shows the considerable weight that the masculine gender on the risk of occurrence of cardiovascular events and the protective nature of estrogen-progestin hormones in women.
Indeed in our series women had cardiovascular events at an older age than men in all categories except ischemic heart disease. The most common cardiovascular risk factor was high blood pressure with 71% of cases. It is indeed the risk factor most correlated with the occurrence of stroke, furthermore it increases the risk of heart failure by 4 and that of myocardial infarction by 3; associated with other risk factors it is multiplied by 20 [4]. Its heavy weight on the occurrence of cardiovascular events and its very high prevalence in the general population explains these data.
Head CT was performed systematically in all patients admitted for focal deficit and / or aphasia, it was normal in 14% of cases and showed ischemic stroke in the rest of the cases. This result corroborates the data from the literature where we find 80% [5].
The clear predominance of cerebrovascular accidents is related to the multiplicity of cardiovascular risk factors that cause infarction [6]. An ejection fraction of less than 30% at echocardiography, was found in 10% of patients as in 29% of heart failure patient.
During hospitalization, 95% of our patients had favorable outcome and 5% died. This conclusion is much more favorable than that obtained in a series where 10% died during hospitalization [3].
In contrast to the length of hospital stay which was much shorter in the pilot study (4 days) than in ours where it is 8.6 days [7]. It is indeed a major criterion for the evaluation of diagnostic and therapeutic performance.
Conclusion
Cardiovascular diseases are more and more frequent with male predominance. The length of hospital stay and the mortality rate remain high. Therefore, an improvement of the management of these cardiovascular pathologies is necessary and works primarily by the control of the modifiable cardiovascular risk factors in particular the scourge which constitutes arterial hypertension but also by the development of the equipments guarantee of speed and efficiency of care.
References
- Baudin B, Cohen A. Données épidémiologiques des maladies cardio-vasculaires et prise en charge des accidents cardiovasculaires. Rev Fr des labo. 2009; 409: 27-39.
- https://www.who.int/fr
- Antignac M, N’guetta R, Macquart De TD, et al. Etude février: Observatoire des hospitalisations en service de cardiologie de l'Afrique subsaharienne : Résultats de l’étude PILOTE sur 103 hospitalisations en Côte d’Ivoire. Cardiol tropical. 2013; 143: 167.
- André P, Six M, Grison C, et al. Interest of a physical activity adapted for the correction of the factors of cardiovascular risk at the coronary subject. Kinesither Rev. 2013; 13: 23-28.
- DARA GJ. Diagnosis of ischemic stroke. The american journal of Medecin. 2009; 122: 14-20.
- Bourrier P. Les AVC dans le service d’accueil et d’urgence (Conférence de consensus) Nice le 4 avril. 1997.
- Juillière Y, Trochu JN, de Groote P, et al. Heart failure with preserved systolic function : a diagnostic algorithm for a pragmatic definition. Arch Mal Cœur. 2006; 99: 279-286.