Twin Pregnancies Revealing Rheumatic Mitro-Aortic Poly-Valvulopathies in a 20-Year-Old Woman in Cardiology CHU Ignace Deen from Guinea Conakry
Author(s): Soumaoro Morlaye1, Samoura Aly1*, Samoura Sana1, Camara Abdoulaye1, Barry Ibrahima Sory1, Diallo Yaya2, Koivogui Diara1, Doumbouya Mohamed1, Balde Elhadj Yaya1, Beavogui Mariama1, Balde Mamadou Dadhi1 and Conde Mamady1
1Cardiac Service Ignace Deen CHU Conakry, Guinea.
2Maternity service Ignace Deen CHU Conakry, Guinea.
*Correspondence:
Samoura Aly, Cardiac Service Ignace Deen CHU, Conakry, Tel: 224 622 104 550/666 753 858.
Received: 24 June 2019; Accepted: 28 July 2019
Citation: Soumaoro Morlaye, Samoura Aly, Samoura Sana, et al. Twin Pregnancies Revealing Rheumatic Mitro-Aortic Poly Valvulopathies in a 20-Year-Old Woman in Cardiology CHU Ignace Deen from Guinea Conakry. Cardiol Vasc Res. 2019; 3(4); 1-3.
Abstract
Objective: Introduction :The heart disease seen in pregnant women is rare but serious, representing the leading cause of maternal mortality in the UK registry [1]. In western countries, valvulopathies account for a quarter of the heart diseases observed during pregnancy, the most common being congenital heart disease [2]. Even in Western countries, these valvulopathies are most often of rheumatic origin. They remain by far the most common heart disease in developing countries [3].
Observation: It was M B 20 years housewife size = 1.64 m, weight = 69 Kg admitted for dyspnea class II, palpitations, physical asthenia and edema of the lower limbs. Evolving for 1 month without risk factor of known cardiovascular disease, with a history of hypertensive mother for 8 years under IEC, it is also followed in maternity for evolutionary twin pregnancy of 32 SA according to the prenatal consultation book (ANC) and biometrics (ultrasound obstetric).
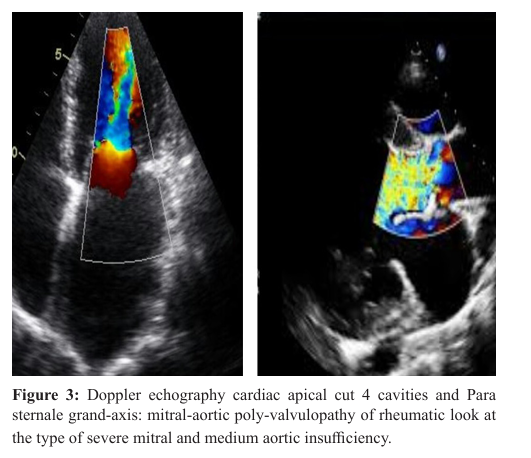
On physical examination the shock tip is visible and palpable at the 5th intercostal space left on the medio clavicular line, peripheral pulses are well perceived fast. SPO2 = 98% in the ambient air, heart sounds are regular at 87 bpm approximately TA 120/80 mmHg a systolic murmur of 4/6 in the mitral focus radiating to the left armpit and a diastolic murmur at the aortic focus radiating along the left edge of the sternum.
To the lungs the vocal vibrations are transmitted, the vesicular murmurs are audible, Abdomen increase in volume there was an ovoid uterus with a long longitudinal axis and a large upper end no uterine contraction with a uterine height of 20 cm, Musculoskeletal edema is noted to the lower limb soft bilateral painless not keeping scoop The rest of the examination is without particularity.
Conclusion: In conclusion, the presence of a valvulopathy, and even more of a polyvalvulopathy, in a pregnant woman requires an individualized evaluation because the risk of gravidic complications is variable according to the type of valvulopathies and their tolerance. Stenosing valvulopathies, especially mitral, require special vigilance, with monthly monitoring from the second trimester in the cardiologist before delivery.
Keywords
Introduction
The heart disease seen in pregnant women is rare but serious, representing the leading cause of maternal mortality in the UK registry [1]. In western countries, valvulopathies account for a quarter of the heart diseases observed during pregnancy, the most Volume 3 | Issue 4 | 1 of 3 common being congenital heart disease [2]. Even in Western countries, these valvulopathies are most often of rheumatic origin. They remain by far the most common heart disease in developing countries [3]. Valvulopathies represent a heterogeneous group by the type of lesions and their prognosis during pregnancy. The analysis of the polyvalvulopathies must be individualized according to the type, the severity of each valvulopathy and their tolerance. Lastly, patients previously operated on pose problems inherent to the type of valvular substitute
Observation
It was M B 20 years housewife size = 1.64 m, weight = 69 Kg admitted for dyspnea class II, palpitations, physical asthenia and edema of the lower limbs. Evolving for 1 month without risk factor of known cardiovascular disease, with a history of hypertensive mother for 8 years under IEC, it is also followed in maternity for evolutionary twin pregnancy of 32 SA according to the prenatal consultation book (ANC) and biometrics (ultrasound obstetric). On physical examination the shock tip is visible and palpable at the 5th intercostal space left on the medio clavicular line, peripheral pulses are well perceived fast. SPO2 = 98% in the ambient air, heart sounds are regular at 87 bpm approximately TA 120/80 mmHg a systolic murmur of 4/6 in the mitral focus radiating to the left armpit and a diastolic murmur at the aortic focus radiating along the left edge of the sternum. To the lungs the vocal vibrations are transmitted, the vesicular murmurs are audible, Abdomen increase in volume there was an ovoid uterus with a long longitudinal axis and a large upper end no uterine contraction with a uterine height of 20 cm, Musculoskeletal edema is noted to the lower limb soft bilateral painless not keeping scoop The rest of the examination is without particularity.
Biology
Hematoxylates = 3.2 T, Hemoglobin = 11 U / L, Hematocrit = 35%, VGM = 75.7 μL, TCHM = 23.7 μg / GR, MCHC = 29.1%, Leukocytes = 22, Lymphocytes = 2, 7, Neutrophils = Platelets = HIV = negative, AgHbs = negative, Fasting blood glucose = 0.90 g / l, Urea = Creatininemia = 1.2mg / dl, Transaminases GOT = 3.01, GPT = 34.12, Calcemia = 5.34, Magnesium = 1.39, Blood Ionogram: Chlorine = 107.32, Potacium = 3.3, Sodium = 5.33, TE = negative, ASLO = positive, CRP = 64 IU, GE + dp = Positive Plasmodium, Widal TO = 1/400 IU, TH = 1/400 IU

Impotent sounding on the left cardiac cavities. Good biventricular systolic function FE = 68% in Teicholz; TAPSE = 25mm.
Discussion
The polyvalvulopathies encountered in pregnant women are mainly of rheumatic origin in 65% of cases [4]. Our result is similar according to data from the literature that states that the major part of the rheumatic vasculopathies. The most common complications of rheumatic fever are mitral stenosis (MR), and aortic insufficiency (RA), and the combination of MR and AI is the most frequently encountered polyvalulopathy [4]. Our series is different from that of LUNG B et al in 2015, which found a predominance of mitral stenosis and aortic insufficiency The coexistence of an AI invalidates the assessment of the severity of RM by the half-pressure time. Pregnancy is associated with sinus tachycardia of approximately 10 additional beats per minute, resulting in shortening of refractory periods and acceleration of conduction velocities especially atrial fibrillation complete arrhythmia its frequency is 5% and thromboembolic risk is similar other subjects and depends on the duration of the arrhythmia and underlying cardiac disease. In our case, there was an electrical anomaly of myocardial ischemia type in the extended anterior recorded by the electrocardiogram.
frontal chest x-ray, which showed cardiomegaly with an ICT = 0.66, no parenchymal or bronchial involvement. Cardiac echinoppler, the latter can detect the severity of heart failure, detect valvular lesions and their severities, look for anomalies related to the three tunics
The management of polyvalvulopathies is difficult in the general population because each combination of valvulopathy has specificities concerning echocardiographic evaluation and indications of intervention [6]. In our study she was treated with the aim of improving the congestive signs of heart failure secondary to valvulopathies such as a diuretic of lanse Lasilix 80 mg divided into two doses per day, an ACE inhibitor (Coversyl 5mg / j) and an anti-aldosterone (Aldactone 25mg / d), and Bisoprolol 5mg per day divided into two doses in bones. The evolution was favorable after 8 days of medical treatment with regression of the congestive signs of heart failure and antibiotic therapy with Penicillin V two girlfriends divided into two doses in bones.
Obstetrical complications are indeed more frequent in patients with heart disease and the occurrence of intrauterine growth retardation can lead to anticipate the date of delivery [4].
In our study at 35th week of amenorrhea she went back to work and the delivery was led by the midwife mothering motherhood by vaginally uncomplicated both male newborns with the following parameters: respective births of 2,100kg and 1,900kg, a respective blood glucose level of 0.98mg / l and 0.95mg / l a SpO2 = 98%, 97% to ambient air, respective size 48cm to 46cm, the respective cranial perimeter of = 29 cm and 31cm and breastfeeding for natural breastfeeding.
Conclusion
In conclusion, the presence of a valvulopathy, and even more of a polyvalvulopathy, in a pregnant woman requires an individualized evaluation because the risk of gravidic complications is variable according to the type of valvulopathies and their tolerance. Stenosing valvulopathies, especially mitral, require special vigilance, with monthly monitoring from the second trimester in the cardiologist before delivery. Valvulopathy should ideally be evaluated and treated before pregnancy. Indications for valvular surgery should remain exceptional during pregnancy because of the fetal risk. Surveillance and planning of delivery should be based on multidisciplinary care.
References
- Thorne SA. Pregnancy in heart disease. Heart. 2004; 90: 450456.
- Roos-Hesselink JW, Ruys TP, Stein JI, et al. Outcome of pregnancy in patients with structural or ischaemic heart disease: results of a registry of the European Society of Cardiology. Eur Heart J. 2013; 34: 657-665.
- Diao M, Kane A, Ndiaye MB, et al. Pregnancy in women with heart disease in sub-Saharan Africa. Arch Cardiovasc Dis. 2011; 104: 370-374.
- Lung B. au Département de cardiologie, hôpital Bichat, université Paris Diderot, 46, rue Henri-Huchard, 75018 Paris, France Disponible en ligne sur ScienceDirect le 10 novembre 20155
- Dacosta A Roméyer-Bouchaud C, Bisch L, Khris L, et al. la fibrillation auriculaire enjeux épidémiologiques, définition, nosologie, medico-économique. Annal de cardiologie et d’angiologie. 2009; 51: 3-5.
- Unger P, Rosenhek R, Dedobbeleer C, et al. Management of multiple valve disease. Heart. 2011; 97: 272-277.