Using Artificial Intelligence to Simulate Brain Function, Enhance the Etiology of Diabetes and Cancer, and more Precisely, Effectively and Remotely Screen and Treat the Patient
Author'(s): Graham Wilfred Ewing B.Sc*
Mimex Montague Healthcare Limited, Mulberry House, Nottingham, United Kingdom.
*Correspondence:
Graham Wilfred Ewing, Mimex Montague Healthcare Limited, Mulberry House, 6 Vine Farm Close, Cotgrave, Nottingham NG12 3TU, United Kingdom.
Received: 02 April 2020 Accepted: 30 April 2020
Citation: Graham Wilfred Ewing. Using Artificial Intelligence to Simulate Brain Function, Enhance the Etiology of Diabetes and Cancer, and more Precisely, Effectively and Remotely Screen and Treat the Patient. Diabetes Complications. 2020; 4(2); 1-8.
Abstract
The steady emergence and evolution of Artificial Intelligence technologies is an area of mathematics which holds immense promise for healthcare. As the body’s physiological parameters are immensely and finely regulated it can, in principle, be mathematically modelled if the mechanism by which the body functions can be understood. This was first achieved by Grakov during the period 1981-1997 when he created a mathematical model of the relationship between sense perception, brain function, the autonomic nervous system and physiological systems, and cellular and molecular biology - which can be used to screen and treat the patient. The author discusses in this
paper how this cognitive technology - known by the brand name ‘Strannik’ - can, in principle, be used to advance the etiology of a wide range of pathologies including diabetes, diabetic comorbidities and cancers; and how it may offer a means of remotely (online) screening and treating patients in the post-CoVid-19 world.
Keywords
Introduction
The term Artificial Intelligence is much abused. It implies that techniques can be developed which have the capability of independent thought, or ‘intelligence’, however most AI type techniques merely use observed patterns in the data and of mathematical formulae and/or algorithms which can improve the performance of existing methods or technologies.
Computers have been programmed to beat the most intelligent chess ‘grand masters’ yet it is not the computer which has intelligence. It was the team of programmers which developed the computer programme who, by virtue of their programming work, gave the computer the capability of being able to solve complex problems on the chess board.
The same applies in healthcare, where Artificial Intelligence (AI) is being used to enhance the diagnosis of pathological anomalies identified by radiological tests yet this assumes that the identified pathological anomaly is an accurate determinant of the condition. They are often based upon the prevailing etiology of the medical condition which in many cases remains poorly defined. The evidence illustrates that this often leads to misdiagnosis or the misidentification of, for example, non-carcinogenic and/or carcinogenic lumps, tumours, etc [1]. It indicates the need for a screening technique which can identify and/or measure the pathological nature and/or significance of the anomaly rather than merely determining its physical parameters. Consider what could be possible if it were possible to mathematically model the relationship between brain function and pathological onset.
The term ‘Artificial Intelligence’ suggests the presence of a greater form of intelligence than has been incorporated into the original radiological device yet such devices invariably incorporate a range of mathematical devices and/or techniques to make sense of the scanned data and thereby enable the technology to scan for a pathological anomaly therefore, in this context, AI is therefore the ‘line extension’ of the radiological device which can be used to enhance the image created.
The value of such scans and tests is to confirm a diagnosis and identify the location of the abnormality prior its surgical removal. This illustrates the undoubted value of the technology but also its limitations e.g. if the lump is benign. Ideally we would wish to have (i) an inexpensive screening modality which would determine in precise detail the medical nature of the abnormality rather than using such highly expensive scanning modalities in a screening capacity; (ii) a scanning modality which determines the physical location of the abnormality(s); and (iii) a safe, non- surgical therapeutic intervention which would reverse or otherwise entice the diabetic symptoms and the lump, bump and/or tumour to regress to a benign state and/or no longer be significant. The diabetic symptoms, lump and/or tumour formed as a result of a particular set of pathological processes so what can be done to reverse this process(es)?
No-one knows what the post-CoVid-19 world of medicine will look like in several months. Perhaps the world will never be the same and remote methods of screening and treating the patient may be required.
Could knowledge of how the brain regulates the autonomic nervous system and/or the coherent and stable function of the physiological systems be significant?
It takes a significant array or spectrum of genetic mutations and polymorphisms, which influence the genetic expression of pre- pro-insulin and subsequent pathways, to influence the metabolism of blood glucose. This is significant because elevated levels of blood glucose are considered to influence the onset and growth of cancers [2].
Genetic screening has been used to identify the genotype for various cancers, in particular how patients with mutations of the BRCA1 and BRCA2 genes [3] have greater predisposition (30- 70%) to cancer [4,5] but many lifestyle-related factors (phenotype) such as excess weight [6-8], the aging process [9], consumption of alcoholic and acidic beverages [10,11], exposure to psychological stress [12]; are also linked to the predisposition to a wide range of conditions including diabetes, diabetic comorbidities, cancer, etc. Accordingly, the identification of BRCA1 or BRCA2 mutations cannot be considered to be a definite indication of the cancerous process [4] and must be components and/or indications of a much broader process [7].
So, what do these factors – excess (or lower) weight, becoming older/elderly (age), the consumption of alcoholic drinks, and psychological stress - have in common?
All pathologies, without exception, have a genetic and phenotypic (stress-related) component. This is what we know and/or recognise as the parasympathetic and sympathetic nervous system(s) resp. In some cases the pathology can have genetic origins which will stress the patient, and in other cases psychological stress is almost solely responsible for pathological onset [12,13], however in most, if not all, cases pathological onset has both genetic and phenotypic components i.e. the genetic process and the non-genetic/phenotypic process are comorbidities.
This is particularly evident in diabetes where the genetic expression of pre-pro-insulin (the chemical reaction by which the genes produce pre-pro-insulin) is followed by a sequence of processes including the reaction of insulin with its receptor protein (type 2 diabetes). It is therefore eminently logical that type 1 diabetes can occur without being accompanied by type 2 diabetes, and that type 2 diabetes can occur without being accompanied by type 1 diabetes, but also that both processes often occur as comorbidities [14,15].
We know from genetic screening that it often takes many genes to express a protein [17,18] and that the genetic spectrum which expresses a protein e.g. insulin, may differ between racial subtypes [19]. So the genetic profile of the diabetic patient can differ, perhaps significantly, yet the protein will still be expressed therefore there is much more to be considered than just the array of genes. In the case of type 1 diabetes changes to genetic structure occur (mutations, alleles, polymorphisms) which alter genetic conformation [20] and thereby alters the energetics of the genetic profile, and hence the genetic expression of pre-pro-insulin, but as yet there is not a cost-effective way of interpreting which genes actively influence this process. Moreover when genetic variations are identified it is reasonable to consider whether they cause the condition or whether they are the consequence of the condition e.g. elevated levels of transition metals contribute to free radical processes [21,22] which influence our genetic profile.
In type 2 diabetes insulin ‘resists’ reacting with its substrate. This is called ‘insulin resistance’ but such a phenomenon is not unique to insulin. Other proteins are known to ‘resist’ reacting [23] under pathological conditions however to describe the phenomena in such terms is an extraordinary way of describing the reaction kinetics of this chemical reaction i.e. that the reaction of insulin with its receptor protein cannot proceed to completion in the expected manner under the prevailing reaction conditions. The primary reaction of insulin with its receptor protein declines and/ or is less efficient and side-effects occur. The question arises why this should be so.
If we delve further into the matter, we find that the reaction of insulin with its receptor protein is dependent upon four issues which have common origins. Pathological onset rarely occurs when intercellular pH is maintained at ca 7.35. It illustrates that the prevailing level of intercellular pH adversely influences (i) the level and/or reactivity of transcriptases, which are often dependent for their activity upon the prevailing levels of magnesium and zinc, and which catalyse the expression of insulin; (ii) insulin conformation and reactivity which is pH dependent; (iii) the prevailing level of magnesium which catalyses the reaction of insulin with its receptor protein [24,25]; and (iv) the storage and/ or reactivity of zinc.
The reaction of insulin with its receptor protein is a magnesium dependent reaction - but it does not explain how diabetic symptoms occur in patients with normally functioning pancreas’ [26,27]. Elevated levels of acidity have the effect of lowering the prevailing levels of essential minerals (for example the reaction of magnesium with phosphoric acid to form insoluble magnesium phosphate salts or the reaction with zinc salts and acetic acid to form insoluble, or sparingly soluble, zinc acetate salts) and elevating the levels of transition metals which are catalysts of free radical reactions [28] and alter the genetic profile and subsequent expression of proteins, the reaction of proteins to form glycated metabolites, the onset and progression of cancerous tumours [29,30], function of the immune response [31,32], etc.
Altering intercellular pH e.g. through the biological buffer Metformin [33], does not prevent the onset of diabetes, or the onset of diabetic comorbidities, or cancer but it does inhibit their further development. In the case of cancer: cancerous cells proliferate in an acidic environment which is not conducive to immune cells [30] therefore neutralizing elevated levels of acidity e.g. with sodium bicarbonate, increases the level of immune response provided by t-cells and enhances the effectiveness of cancer treatments. It begs the question whether sodium bicarbonate alone could be an effective remedy against pathological onset, in particular, where diabetes and cancer is concerned.
Non-pancreatic diabetes occurs in patients with pathological indications in the hypothalamus [34] and the primary endocrine glands - pituitary, thyroid and adrenals [35-38] - in females who have had a hysterectomy [16] and probably also in males with prostate problems. It illustrates that emergent pathological indications in the endocrines and sexual organs must in some way influence the process i.e. that pathological onset in the pancreas is worsened by pathological onset in other organs and other organ networks.
So how can we explain these phenomena?
Diabetes Mellitus is the term which we use to describe the regulation of blood glucose levels between upper (hyperglycaemia) and lower (hypoglycaemia) limits. The evidence clearly illustrates that the process - the regulation of the autonomic nervous system and physiological systems, and in particular the regulation of blood glucose levels, is neurally regulated. In other words what we know as Diabetes Mellitus is only part of the problem. So how can we measure the complex nature of diabetes as outlined in this paper? In particular, how can we measure the rate of reaction of the various pathologies which influence the regulation of blood glucose?
At first glance this appears to be impossible. We can identify, by genetic screening, the genes and genetic mutations which collectively interact to express insulin although genetic research does not yet recognise, at least publicly, why and how this occurs. Biomedicine does not have – or does it? - a technology which can precisely measure the rate and/or level of genetic expression of insulin and it does not have a screening technology which can accurately screen and/or measure the phenotype. It is reasonable to consider, therefore, whether there is a phenomena upon which such a technology could be based.
Diabetes is characterized by changes of colour perception [39-43] and brain function. Many researchers have sought unsuccessfully to adopt these phenomena, and develop a diabetes diagnostic test, perhaps for reasons outlined in this paper. The phenomena is based upon the observation that changes of colour perception have pathological origins i.e. that the emission of biophotons of light, hitherto known as bioluminescence, accompanies pathological onset and is a direct measure of rate of reaction of every pathological process. It presents an opportunity to develop a technology which can determine both the genotype and phenotype (the stress response) for every common pathology including those which influence the regulation of blood glucose levels. The idea of using such phenomena as the basis of a diagnostic technique is not new [44,45].
At first glance this may seem like a dream, fantasy or illusion of what could be possible however a technique or combination of techniques has already been developed by leading geneticists, and respected researchers, which can screen both the genotype and phenotype [46] for all common pathologies in all of the 30 main organs throughout the body system. Moreover the Human Brain Project was created – at a cost of EUR1.2BN - with the specific intention of understanding this phenomena.
The common/historical way of screening for diabetes is based upon measuring the level of blood glucose, using FG and/or OGTT, and glycated haemoglobin (HbA1c) however the measurement of HbA1c is based upon a series of assumptions and as a result is fraught with inaccuracies [47,48] due to a wide range of factors e.g. pH, exposure to light, levels of haemoglobin, blood cell count, etc. It fails to consider that the rate of glycation is multifactorial, that the production/ratio of the different glycated isomers varies according to the prevailing reaction conditions, and hence that the level of the A1c isomer cannot be an accurate indication of diabetes e.g.
- It is possible to have abnormally low or elevated levels of blood glucose and to have nothing wrong with your pancreas - non-pancreatic diabetes.
- It is possible to have elevated levels of blood glucose and yet our levels of glycated haemoglobin may be significantly lower (or higher) than expected norms.
- The stress response influences the management of type 1 diabetes [49].
- Type 1 and 2 diabetes occur as comorbidities [50].
If we do not understand what is diabetes, and hence what causes diabetes, how can it be possible to make significant improvements to the healthcare system to address this problem?
Using such a technology – known by the brand name Strannik - we can now measure the precise systemic characteristics and/ or correlates of pathological onset and identify which organs are involved, the pathological spectrum in each organ, and the level of genotype and phenotype for each pathology, etc. (Figure 1). The statistics, obtained from 15-20 clinical studies which have been conducted in Russia, Spain and South Africa [51]; illustrate that Strannik Virtual Scanning (SVS) is ca 2-23% more accurate than the entire range of diagnostic tests against which it was compared and which were in use in the various test clinics. This is the order of magnitude which could be expected if indeed the SVS test is based upon a precise understanding of how the brain regulates the autonomic nervous system and, in particular, if it was able to accurately determine the degree of pathological onset in the various pathologies which characterize the patient’s medical condition.
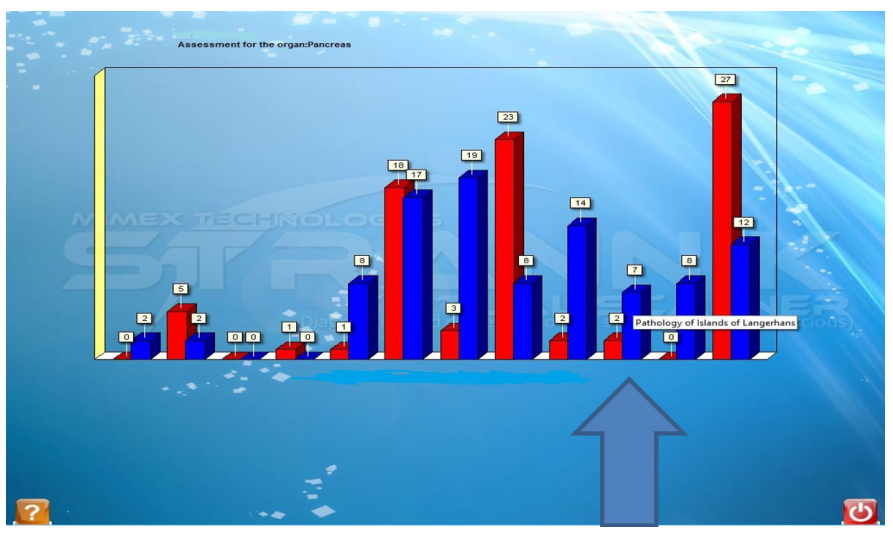
Figure 1: Strannik Virtual Scanning Test Report.
Interpretation of Results
Each blue/red pair is indicative of the genetic or phenotypic characteristics of each individual pathological indication e.g. in the above report for the Pancreas: diabetes (pathology of the islets of Langerhans), pancreatitis, sclerosing pancreatitis, growth of new cells, allergic process, etc. The arrow highlights the diabetes signal. A patient with 25 units (blue/genotype) would be experiencing significantly reduced expression of insulin (Type 1DM). For example: (i) a patient with 25 units (red/phenotype) would be experiencing increased ‘insulin resistance’ i.e. reduced levels of insulin reactivity (type 2DM); (ii) patients with for example 20 units genotype and 28 units phenotype would be experiencing a combination of the two diabetic subtypes. In the case of cancer, for each organ, the indication of ‘growth of new cells’ would be indicative of such pathology(s).
Report
This particular patient has reduced expression of insulin (7 units(blue)) and low phenotype (2units(red)) which are at presymptomatic level (below 10 units) for both type 1 and type 2 diabetes i.e. the patient has pre-T1 diabetes.
Note
This report illustrates how the SVS test determines (i) pathological onset from its pre-symptomatic origins, (ii) the genetic and phenotypic nature of each pathology, and (iii) determine ca 15 pathological indications in each of the 30 main organs. Each is highlighted as a pop-up title when ‘the mouse’ hovers over the particular pathology of interest.
Such an Artificial Intelligence technique - based upon a mathematical model of the relationship between sense perception (in particular of colour perception), brain function, the autonomic nervous system and physiological systems, and cellular and molecular biology - offers a scientifically consistent, valid, sophisticated and relatively inexpensive way of screening for the range of pathological indications which influence blood glucose levels including what we commonly refer to as type 1 and type 2 diabetes.
Changes of molecular biology influence cell biology, which in turn influences the structural integrity of the organs, however the organs are component in organ networks which are commonly known as physiological systems. This raises the fundamental question: how are these organ networks regulated? Biology and/or biomedicine alone cannot explain this phenomenon.
To explain this phenomenon we must turn to neuroscience [52]:
- If we eat and drink too much of the wrong things and exercise too little [53] we will inevitably, and in due course, develop a plethora of ailments which influence all aspects of the body’s function including diabetes, obesity and cancer;
- Stress is experienced through the senses and influences the brain’s ability to regulate what we eat, how we eat, the quantities consumed, the quality of our sleep, etc;
- The integrity of our genetic profile is influenced by viruses, virus-like particles, intercellular pH, and exposure to free radical species (ROS); and
- The body is a highly regulated entity which is influenced by the relationship which exists between our genotype and our The nature of this relationship is that it influences the stable and coherent function of the autonomic nervous system and physiological systems.
The brain regulates appetite, hunger, satedness [54]. It functions as a neuromodulator which continuously regulates the stable and coherent function of the autonomic nervous system and physiological systems [55] i.e. by the stress response which is processed via the senses.
What are the mechanisms by which the brain modulates the stable and coherent function of the physiological systems?
The brain’s function can be influenced by magnetic and electrical impulses, frequency, exposure to sensory input, changes to genetic profile and by pharmacological input. This mechanism involves the vagus nerve although there are doubts that the vagus nerve is the sole pathway because it must involve the pituitary and thyroid glands which secrete various hormones directly into the blood via the blood vessels.
Moreover, the mechanism by which we develop diabetes and obesity usually involves us exercising too little or eating and drinking too much of the wrong things so the fundamental mechanism by which we develop diabetes and obesity is psychological and/or neurological. Accordingly, any proposed mechanism should be based upon a phenomenon – an understanding of nervous system activity - which incorporates all of these factors [56,57]. This is the function of the neural frequencies which are measured by electroencephalograph and which regulate the stable and coherent function of the organs and/or organ networks (physiological and/ or functional systems. It is particularly significant because blood glucose is a neurally regulated physiological system (network of organs) i.e. the body is a biological entity which fuels a biophysical entity - the brain - therefore pathological onset influences the ability of the brain to perform its essential function of maintaining the body’s physiological stability. This instability is responsible for what we know and experience as pathological onset or progression. A precise understanding of this mechanism would enable healthcare to treat the fundamental (psychosomatic) causal mechanisms AND the symptomatic (somatic) presentation of the person’s unique medical conditions.
The brain uses frequency to govern, influence and/or manage the multi-level nature of brain function and regulate the coherent function of the autonomic nervous system and physiological systems e.g. of blood glucose levels [58-60]. Knowledge of this mechanism can be used to regulate the stable and coherent function of each of the body’s 13 physiological systems. It explains why the selection of the wrong parameters can lead to the onset of photosensitive events e.g. by stimulating reductions in blood flow and/or the flow of oxygen to the brain, as occurs in complex medical syndromes e.g. migraine, epilepsy or depression [61-63].
Pathological onset is the consequence of the process by which biological input AND multi-sensory input influence brain function i.e. the neural and visceral data matrices operate dynamically. Changes of diet, stress and environment influences this dynamic and ultimately the body’s function and is manifest as a spectrum of pathologies which influences blood glucose levels, heart function, breathing, kidney function, pancreatic function, sleep, etc.
It illustrates the existence of a set of organizational principles which the brain, through its control of nervous system activity, deploys to regulate the body’s function. Moreover, the outcome of this process is changes of how we behave – of memory, alertness, vitality, speed and smoothness of movement; how we learn; how and why we are tired and need sleep; our ability to create relationships; how we organize our lives and our priorities throughout the day, weeks and months ahead; our effectiveness i.e. our ability to start and complete the many tasks which we require to complete each day; etc.
As outlined, pathological onset influences the brain’s ability to regulate the coherent function of the organ networks including blood glucose levels. In order to do so the brain functions as a neuromodulator which uses the EEG frequencies to modulate the coherent function of the organ networks i.e. pathological onset influences brainwave coherence and vice versa. Different components work at different frequencies i.e. the precise nature and degree of pathological onset in the patient influences the selection of modulating frequencies, dose responses, etc.
The mathematical model created by Grakov, as outlined in this and many other papers, is able to determine the stability of the body’s physiological systems and hence recognize which systems are most dysfunctional. This enabled Grakov to adapt Anokhin’s research and determine the parameters for the Strannik Neuromodulation Therapy (SLT) which initial research has illustrated is 75-96% effective and which compares with the ca 50% effectiveness of most common drugs [64].
Such developments in medicine are rare and considered often to be quite incredulous, particularly so by sceptical proponents of biomedicine nevertheless various neuromodulation techniques are being increasingly used to treat medical conditions which cannot be effectively treated using pharmacological medications.
Patient male 65+ years, internationally respected doctor of medicine, type 1 diabetic/diabetic leg ulcer:
Quote: ‘This simple easy, pain free test then allowed her (Dr Elena Ewing) to diagnose 5-15 pathologies in each of the 30 main body organs (e.g. Heart, Liver, Pancreas, etc.), but also on the cellular and molecular levels. I was astounded to have her detect all my major health issues. Diabetes, Heart Disease, etc. This is then followed by a therapeutic exercise which involves passively watching the colored screen for 20 minutes, once or twice per day, which corrects the autonomic dysfunction associated with the person's ill health.
I focused on Diabetes initially as I am Insulin dependent, and my insulin requirements decreased 20-25% over 2 months. I had been taking antibiotics to treat a diabetic leg ulcer. No matter what I had tried it would not heal. I was struggling to manage this problem. Now it started to heal and I am now largely free of this impediment. It can affect more than one system as well as I noticed my muscle pain and weakness due to myopathy was improving. I could also target other specific issue with a separate therapy plan. The Strannik software is simple to use, is diagnostic, and therapeutic simple, painless, easy to use. You will love Strannik therapy.
The Strannik Neuromodulation Therapy is the most advanced of the many neuromodulation and/or biofeedback techniques which are being shown to have significant therapeutic potential. These techniques have been deployed with some success for the last 100 years [65]. In recent years researchers at major universities, in particular in the US, are now employing with steadily increasing levels of success [66] a rudimentary and/or experiential understanding of such principle(s). Perhaps the future of biomedicine requires that it embraces an understanding of how the whole body functions [55,67].
In summary
Diabetes and cancer(s) are what we experience as the symptomatic expression of complex, multi-systemic, multi-pathological and polygenomic disorders. They are part of the complex etiology associated with the neural regulation of the physiological systems including, in this case, the neural regulation of blood glucose level(s) and the growth of new cells which accompany carcinogenic processes and which arise from systemic dysfunction and/or autonomic dysfunction.
The observation that changes of colour perception accompany the onset and progression of changes of blood glucose is significant because it arises from the emission of biophotons in the blood [45] which accompany the onset and progression of complex pathological processes i.e. the emission of biophotons in the retina influences brain function. It is a digital phenomenon which, in principle, can be used as a more precise and sophisticated way of measuring pathological onset than by measuring levels of biochemical components. It is a form of Artificial Intelligence because (i) it simulates brain function and (ii) all forms of diagnostic measurements are based upon a set of assumptions and have a range of limiting parameters. Nevertheless, initial indications are that this body of knowledge, developed by IG Grakov, represents a more advanced and more precise way of determining and treating patient health than contemporary diagnostic and therapeutic modalities.
References
- Evans AJ, Pinder SE, Ellis IO, et al. Screen detected ductal carcinoma in situ DCIS overdiagnosis or an obligate precursor of invasive disease. J Med Screen. 2001; 8: 149-
- Li W, Zhang X, Sang H, et Effects of hyperglycemia on the progression of tumor diseases. J Exp Clin Cancer Res. 2019; 38: 327.
- Venkitaraman AR. Functions of BRCA1 and BRCA2 in the biological response to DNA damage. Journal of Cell 2001; 114: 3591-3598.
- Ford D, Easton DF, Stratton M, et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer The Breast Cancer Linkage Consortium. Am J Hum. Genet. 1998; 62: 676-689.
- Rahman N, Stratton MR. The genetics of breast cancer Annu Rev Genet. 1998; 32: 95-121.
- Stone TW, McPherson M, Gail Darlington Obesity and Cancer Existing and New Hypotheses for a Causal Connection. E Bio Medicine. 2018; 30: 14-28.
- Wolin KY, Carson K, Colditz GA. Obesity and cancer. 2010; 15: 556-565.
- Colditz GA, Peterson LL. Obesity and Cancer Evidence Impact and Future Directions. Clinical Chemistry. 2018; 64: 154-162.
- White MC, Holman DM, Boehm JE, et al. Age and cancer risk: a potentially modifiable Am J Prev Med. 2014; 46: S7-S15.
- Klein WMP, Jacobsen PB, Helzlsouer KJ. Alcohol and Cancer Risk. Clinical and Research Implications JAMA. 2020; 323: 23-24.
- Zaitsu M, Takeuchi T, Kobayashi Y, et al. Light to moderate amount of lifetime alcohol consumption and risk of cancer in Cancer. 2020; 126: 1031-1040.
- Moreno Smith M, Lutgendorf SK, Sood Impact of stress on cancer metastasis. Future Oncol. 2010; 6: 1863-1881.
- Kruk J, Hassan B, Enein A, et Psychological Stress and Cellular Aging in Cancer A Meta Analysis. Oxidative Medicine and Cellular Longevity. 2019. ID 1270397.
- Ewing GW, Parvez The Multi-systemic Nature of Diabetes Mellitus genotype or phenotype. N Am J Med Sci. 2010; 2: 444-456.
- Jain P, Vig S, Datta M, et al. Systems Biology Approach Reveals Genome to Phenome Correlation in Type 2 PLoS ONE. 2013; 8: e53522.
- Luo J, Manson JE, Urrutia RP, et al. Risk of Diabetes After Hysterectomy With or Without Oophorectomy in Postmenopausal Women. Am J Epidemiol. 2017; 185: 777-
- Nyaga DM, Vickers MH, Jefferies C, et Type 1 Diabetes Mellitus-Associated Genetic Variants Contribute to Overlapping Immune Regulatory Networks. Front Genet. 2018; 9: 535.
- Ram R, Morahan G. Effects of type 1 diabetes risk alleles on immune cell gene Genes. 2017; 8: 167.
- Spanakis EK, Golden Race Ethnic Difference in Diabetes and Diabetic Complications. Curr Diab Rep. 2013; 13: 10.
- Ewing GW. The Interpretation of Genetic Data-Considering the Effect of Changes to Gene Conformation If the facts don’t support the theory change the theory how does this contribute to understanding Diabetes. J Genet Disor Genet 2017; 6: 1-4.
- Phaniendra A, Jestadi DB, Periyasamy L. Free radicals properties sources targets and their implication in various Indian J Clin Biochem. 2015; 30: 11-26.
- Aust SD, Morehouse LA, Thomas CE. Role of metals in oxygen radical reactions. J Free Radic Biol Med. 1985; 1: 3-25.
- Ewing GW. A Different Perspective on Diabetes & Obesity what it is and how it can be measured. Case Reports in Clinical 2018; 7: 269-287.
- Lin CC, Huang YL. Chromium, zinc and magnesium status in type 1 diabetes. Curr Opin Clin Nutr Metab Care. 2015; 18: 588-592.
- Barbagallo M, Dominguez Magnesium and type 2 diabetes. World J Diabetes. 2015; 6: 1152-1157.
- Thorell A, Nygren J, Ljungqvist O. Insulin resistance a marker of surgical Curr Opin Clin Nutr Metab Care. 1999; 2: 69-78.
- Hardt PD, Brendel MD, Kloer HU, et al. Is Pancreatic Diabetes Type 3c Diabetes Underdiagnosed and Diabetes Care. 2008; 31: S165-S169.
- Swaminathan S, Fonseca VA, Alam MG, et al. The Role of Iron in Diabetes and Its Complications. Diabetes Care. 2007; 30: 1926-1933.
- Zhang Will cancer cells be defeated by sodium bicarbonate? Sci. China Life Sci. 2017; 60: 326-328.
- Pilon-Thomas S, Kodumudi KN, El-Kenawi AE, et al. Neutralization of Tumor Acidity Improves Antitumor Responses to Immunotherapy. Cancer Research. 2015; 76:
- Tam M, Gómez S, González-Gross M, et Possible roles of magnesium on the immune system. Eur J Clin Nutr. 2003; 57: 1193-1197.
- Li F Y, Lenardo MJ, Chaigne-Delalande B. Loss of MAGT1 abrogates a Mg2+ flux required for T cell signaling and leads to a novel human primary immunodeficiency. Magnes 2011; 24: S109-S114.
- Ewing GW. Is Metformin a Drug or a Buffer and Why is this Significant Further evidence that the brain Regulates the Autonomic Nervous System, in particular prevailing levels of Intercellular pH. Endocrinology, Diabetes and Metabolism 2018; 2: 1-9.
- Chan O, Sherwin Hypothalamic Regulation of Glucose Stimulated Insulin Secretion. Diabetes. 2012; 61: 564-565.
- McCullagh EP, Alivistatos JG. Diabetes of Anterior Pituitary and Adrenal Cortical Diabetes. 1954; 3: 349-357.
- Wendong Liu, Limin Wang, Minghua Liu, et al. Pituitary Morphology and Function in 43 Children with Central Diabetes International Journal of Endocrinology. 2016; 7.
- Hage M, Zantout MS, Azar ST. Thyroid disorders and diabetes J Thyroid Res. 2011; 2011: 7.
- Ullah A, Abouglila K, Ibrahim I, et al. Hyperglycaemia presenting as adrenal insufficiency in type 1 Endocrine Abstracts. 2009; 19: 307.
- Malukiewicz G, Lesiewska-Junk H, Kazmierczak Changes in the colour vision and contrast sensitivity in diabetic patients without retinopathy. Klin Oczna. 2009; 111: 221-223.
- Shoji T, Sakurai Y, Sato H, et al. Do type 2 diabetes patients without diabetic retinopathy or subjects with impaired fasting glucose have impaired colour vision? The Okubo color study Diabet Med. 2011; 28: 865-871.
- Andrade LCO, Souza GS, Lacerda EMC, et al. Influence of retinopathy on the achromatic and chromatic vision of patients with type 2 diabetes. BMC Ophthalmol. 2014; 14:
- Feitosa-Santana C, Paramei GV, Nishi M, et al. Color vision impairment in type 2 diabetes assessed by the D 15d test and the Cambridge Colour Ophthalmic Physiol Opt 2010; 30: 717-723.
- Sun T, Zhang Characters of contrast sensitivity in diabetic patients without male retinopathy. Chin J Ophthalmol. 2012; 48: 41-46.
- Benmiloud F, Godiris Petit G, Gras R, et Association of Autofluorescence-Based Detection of the Parathyroid Glands During Total Thyroidectomy With Postoperative Hypocalcemia Risk Results of the PARAFLUO Multicenter Randomized Clinical Trial. JAMA Surg. 2020; 155: 106- 112.
- https://www2.le.ac.uk/projects/space-ideas-hub/services/tech/bioastral
- https://nytimes.com/2019/05/08/science/precision-medicine-overtreatment.html
- Ed Zhang L. Glycans and Glycosaminoglycans as Clinical Biomarkers and Therapeutics Part A. Progress in Molecular Biology and Translational 2019; 162: 1-400.
- Malka R, Nathan DM, Higgins JM. Mechanistic modeling of hemoglobin glycation and red blood cell kinetics enables personalized diabetes Science Translational Medicine. 2016; 8: 59-130.
- Wiesli P, Schmid C, Kerwer O, et al. Acute Psychological Stress Affects Glucose Concentrations in Patients With Type 1 Diabetes Following Food Intake but not in the Fasting Diabetes Care. 2005; 28: 1910-1915.
- Piette JD, Kerr The Impact of Comorbid Chronic Conditions on Diabetes Care. Diabetes Care 2006; 29: 725- 731.
- Grakov IG, Ewing GW, Mohanlall R, et al. A summary or meta-analysis of data regarding the use of Strannik Virtual Scanning as a screening modality for healthcare. Asian Journal of Pharmacy Nursing and Medical Science. 2017; 5: 55-71.
- Ewing The Future of Medicine: Biomedicine or Neuroscience. Insights in Biomedicine 2016; 1: 14-17.
- van Ommen B, van Keulen HM, Wopereis S, et al. From Diabetes Care to Diabetes Cure The Integration of Systems Biology Health and Behavioral Change. Front Endocrinol 2018; 8: 381.
- Farr OM, Li C SR, Mantzoros Central Nervous System Regulation of Eating Insights from Human Brain Imaging. Metabolism. 2016; 65: 699-713.
- Ewing What is the function of the Brain What does it do and how does it do it It functions as a Neuroregulator which continuously regulates the Autonomic Nervous System and Physiological Systems, and enables us to Recognise that Sleep Exhibits the Characteristics of a Neurally Regulated Physiological System. J Neurol Psychol. 2016; 4: 9.
- Anokhin The Problem of the Center in the Physiology of Nervous Activity. Gorky. 1935; 9-70.
- Khitrov NK, Saltykov AB. Theory of Functional Systems and Human General Pathology. Bulletin of Experimental Biology and 2003; 136: 1-6.
- Hyllienmark L, Maltez J, Dandenell A, et EEG abnormalities with and without relation to severe hypoglycaemia in adolescents with type 1 diabetes. Diabetologia. 2005; 48: 412-419.
- Inui K, Sannan H, Ota H, et al. EEG findings in diabetic patients with and without retinopathy. Acta Neurol Scand. 1998; 97: 107-109.
- Baskaran A, Milev R, McIntyre A review of electroencephalographic changes in diabetes mellitus in relation to major depressive disorder. Neuropsychiatr Dis Treat. 2013; 9: 143-150.
- Dhar AK, Barton Depression and the Link with Cardiovascular Disease. Front Psychiatry. 2016; 7: 33.
- Musselman DL, Evans DL, Nemeroff CB. The Relationship of Depression to Cardiovascular Disease Epidemiology Biology and Treatment. Arch Gen Psychiatry. 1998; 55: 580-592.
- Vaccarino V, Badimon L, Bremner JD, et al. Depression and coronary heart disease 2018 position paper of the ESC working group on coronary pathophysiology and European Heart Journal. 2020; 41: 1687- 1696.
- Spear BB, Heath Chiozzi M, Huff Clinical application of pharmacogenetics. Trends Mol Med. 2001; 7: 201-204.
- Wallace The theory and practice of syntonic phototherapy a review. Optom Vis Dev. 2009; 40: 73-81.
- Martorell AJ, Paulson AL, Suk HJ, et al. Multi sensory Gamma Stimulation Ameliorates Alzheimer’s Associated Pathology and Improves Cognition. Cell. 2019; 177: 256-
- Ewing The Future of Medicine Biomedicine or Neuroscience. Insights in Biomedicine. 2016; 1: 14-17.