Automatic Fetal Heart Rate Monitoring to Prevent Cerebral Palsy with Hypoxia Index
Author'(s): Kazuo Maeda, MD, PhD*
Honorary Professor, Department of Obstetrics and Gynecology, Tottori University Medical School, Yonago, Japan.
*Correspondence:
Kazuo Maeda, Honorary Professor, Department of Obstetrics and Gynecology, Tottori University Medical School, Yonago, Japan, Fax: 81-859-22-6856; E-mail: maedak@mocha.ocn.ne.jp.
Received: 17 July 2018 Accepted: 14 August 2018
Citation: Kazuo Maeda. Automatic Fetal Heart Rate Monitoring to Prevent Cerebral Palsy with Hypoxia Index. Gynecol Reprod Health. 2018; 2(4): 1-3.
Abstract
Aims: To automatically diagnose intrapartum fetal heart rate with the purpose to prevent cerebral palsy.
Methods: Initial system was composed of a minicomputer with paper tape punher/reader and Teletype keyboard, where it diagnosed baseline heart rate and deceleration patterns. Next system was a micro computerized one. Then a centralized one with 50 channel times sharing, composed of FHR score, which predicted Apgar score and UApH. Artificial neural network assesses fetal outcome and frequency spectrum detects ominous sinusoidal heart rate. Novel hypoxia index is the sum of heart rate deceleration durations divided by the lowest heart rate and multiplied by 100.
Results: Perinatal mortality reduced by the central computer. As hypoxia index is 25 or more, if the variability is lost and followed by cerebral palsy, while the fetus is safe not only preventing fetal death, but also preventing cerebral palsy, if the index is 24 or less.
Future: A new computer is planned to recluce asphyxiated neonate and reduces the acidosis by FHR score, to analyze frequency spectrum, and the hypoxia index will prevent infantile cerebral palsy, which will be directly reported doctor.
Keywords
Introduction
Although FHR monitoring is mandatory in the labor management, full visual monitoring of cardiotocogram (CTG) is troublesome during the labor process in 10 or more hours, As it is requested to watch the continuous CTG chart and diagnose possible FHR changes, continuous FHR monitoring, prompt report of abnormal FHR, the most correct diagnosis and the assessment of fetal outcome would like to leave to a computer.
The deceleration pattern classification [1] was the subject of computerized diagnosis in the first study of our automated FHR diagnosis [2], visual impression had to be changed to numeric value, where the baseline heart rate in 5 min was determined by counting FHR data in every 10 bpm steps detecting the most data step, where FHR data in the step were averaged to determine baseline FHR, FHR variations were averaged to achieve long-term variability.
Deceleration pattern classification was complicated, namely, V-shape deceleration was found in periodic deceleration, dip- shape value was determined in every deceleration to classify V shape periodic and U-shape variable decelerations. Basic value is the amplitude (X) and the triangular base width (Y) and deceleration area is the sum of deceleration FHR-baseline FHR (D1-n) multiplied by sampling interval, i.e.

Then the dip area is divided by XY
The deceleration is V shape (early & late decelerations), if dip area <0.5
The deceleration is U shape (variable deceleraion), if dip shape >=0.6
(above 2 equations were obtained by statistics of visual decelerations.)
Te differentiation is complete, if FHR variation is 60 or more in variable deceleration. The calculation was created by Mizu [9].
Lag time was determined between peak of contraction & dip of deceleration in V-shape deceleration:
It is late deceleration, if the lag time is 20 or more sec.
It is early deceleration, if the lag time is less than 20 sec.
Such complicated procedure was needed in the determination of deceleration patterns as above in all decelerations [2]. As the character of late deceleration was vague and uncertain, the pattern classification method was collapsed in computerized monitoring; instead, novel hypoxia index covered all decelerations and continuous bradycardia.
Digital determination of deceleration is very simple if compared above digital translation of visual classification:
- Deceleration area [Cahill et al, 2018] [10] Base width of FHR deceleration x amplitude /2
- Hypoxia index [Maeda, 2018]
Sum of deceleration duration (min) / the lowest FHR (bpm)
Deceleration area was closely related to UApH, while hypoxia index was high in cases of cerebral palsy and low in normal cases, by which cerebral palsy can be prevented. Similar tendency is present among two digital parameters [9].
Methods
FHR score
The FHR score was calculated by the sum of evaluation scores of the FHR baseline and the parts of decelerations by the author, 1969 (Figure 1, Table 1), [3] (Table 2), instead of subjective visual pattern classification.
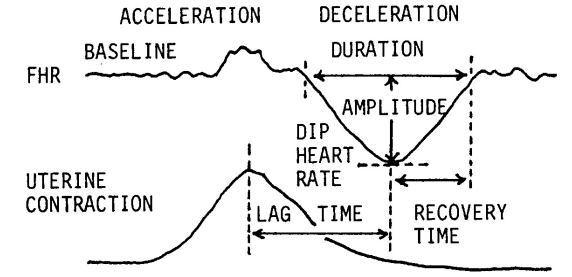
Figure 1: Determination of every parts of FHR changes in objective diagnosis of fetal heart rate curve [3].
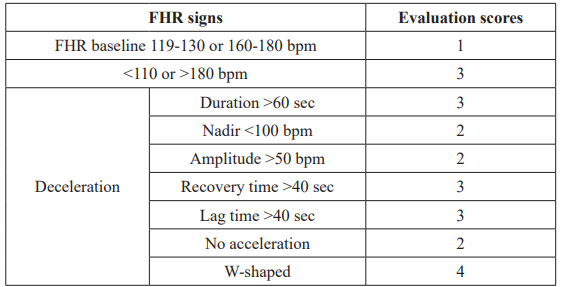
Table 1: Calculation of FHR score. The sum of evaluation scores in 5 minutes achieved FHR score. Evaluation score was decided according to the percentage of low Apgar score lower than 7.
The fetus is abnormal, if FHR score is 10 or more, and highly abnormal if the score is 20 or more.
Results
Fetal outcome was predicted even in the 1st stage of labor as follows by regression equation, i.e. FHR score is useful to indicate early delivery in early stage of labor (Table 2).
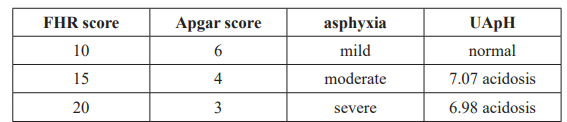
Table 2: Fetal outcome is predicted in the 1st stage of labor according to regression equations.
Hypoxia index
It is a novel FHR index to prevent cerebral palsy, created by the author.
Methods
As intrapartum hypoxic fetal brain damage was caused by frequent repetition of late decelerations as seen in 50 minutes repetition of late deceleration, but not by particular late deceleration pattern as seen in 3 connected late decelerations, thus, the sum of deceleration durations were divided by the lowest FHR, which meant hypoxia intensity.
Hypoxia index is the sum of deceleration durations (min) divided by the lowest FHR (bpm), and multiplied by 100 to be integer, where FHR was calculated instead of PaO2, because heart rate was parallel to PaO2 when PaO2 was lower than 50mmHg [4], and fetal PaO2 was lower than 50mmHg [3], while fetal blood sampling was hard in the labor. Hypoxia index covers all of early, late and variable FHR decelerations, as well as sudden continuous fetal bradycardia.
Results
Fetal hypoxia index (HI) was 25 or more in cases who had the loss of FHR variability and brain damage followed by infantile cerebral palsy, while the HI was 24 or less in the cases who had deceleration but neither fetal brain damage nor infantile cerebral palsy [5] (Table 3).
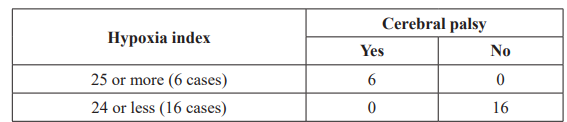
Table 3: Chi square test of hypoxia index and cerebral palsy.
p=0.000008<0.05, significant difference.
Thus, hypoxia index is calculated in computerized fetal monitoring, warning the presence of FHR deceleration, hypoxia index at present and that safe hypoxia index is 24 or less, every 5 minutes.
Frequency spectrum
Frequency spectrum of FHR curves was studied by the authors [6].
Method
Five minutes’FHR curve is always monitored by FHR score, hypoxia index and frequency spectrum, which reports the presence of pathologic sinusoidal FHR when La/Ta ratio is 39 or more and at the same time the PPSD is 300 or more, because pathologic sinusoidal is very ominous by severe fetal anemia close to fetal death. Although there is another benign sinusoidal curve, which was caused by the synchronizlation of FHR to periodic fetal movements, e.g. fetal respiratory movments, but not an ominous sign, only diagnosed by the periodic fetal movements recorded by actocardiogram, and, the false sinusoidal is not reported doctor, thus, the alarm of sinusoidal should not be overlooked in automatic fetal monitoring, because pathologic sinusoidal FHR is always malignant and close to fetal death, thus, urgent caesarean delivery followed by neonatal blood transfusion are performed to cure the baby from the demise.
Discussion
Fetal monitoring should be external method which is able to monitor the fetus before the rupture of membrane in the labor and even in pregnancy., namely, ultrasonic Doppler autocorrelation FHR meter, or abdominal fetal ECG with multiple electrodes excluding maternal ECG will detect FHR curve. FHR computer will be composed in single channel for single pregnant woman, or centralized multiple time sharing system monitorig multiple deliveries. Analyzing program will be the detection of basic FHR components, FHR score to predict fetal outcomes, hypoxia index to predict and prevent cerebral palsy, frequency spectrum analysis to diagnose pathologic sinusoidal heart rate and A/B ratio in actocardiogram, and so on. Quick and direct reporting system to doctor is mandatory for clinical purpose.
Hypoxia Index (HI) is novel and unique in the present study to predict the loss of FHR baseline variability and fetal brain damage followed by cerebral palsy. The hypoxia index=The sum of FHR deceleration duration (min) divided by the lowest FHR (bpm) and multipled by 100, of which purpose is to collect the summation of hypoxic effects in repeated FHR decelerations, where 25 or more of HI predicts the cerebral palsy, and the HI is 24 or less to prevent cerebral palsy.
The data of FHR curve frequency spectrum indicates pathologic sinusoidal FHR showing fetal anemia [6]. A/B ratio is the ratio of FHR acceleration duration to that of fetal movement burst of which value is less than 1 when Apgar score is lower than 7 [7]. The perinatal mortality decreased and cerebral palsy was zero, when there was direct and rapid reporting system in centralized computer [8].
Conclusion
The computerized fetal monitoring improves busy obstetric doctors. Although the caesarean delivery was allowed after the loss of FHR baseline variability in common CTG, namely it prevented fetal death, while it was unable to prevent the cerebral palsy. Early delivery should be performed before the loss of variability to prevent fetal brain damage followed by cerebral palsy [5], while the hypoxia index is 24 or less in the update numeric diagnosis of intrapartum fetal monitoring, where early delivery is performed keeping the hypoxia index at 24 or less level to prevent the loss of variability and fetal brain damage followed by cerebral palsy.
References
- Hon An Atlas of Fetal Heart Rate Patterns. Harty Press, New Haven. 1968.
- Maeda K, Arima T, Tatsumura M, et al. Computer-aided fetal heart rate analysis and automatic fetal-distress diagnosis during labor and pregnancy utilizing external technique in fetal monitoring. MEDINFO 80, North-Holland Publishing 1980; 1214-1218.
- Maeda K, Kimura S, Nakano Pathophysiology of Fetus. Fukuoka Printing, Fukuoka. 1969.
- Umezawa J. Studies on the relation between heart rate and PaO2 in hypoxic rabbit: a comparative study for fetal heart rate change in labor. Acta Obstet Gynecol Jpn. 1975; 28: 1203-1212.
- Maeda K. Modalities of fetal evaluation to detect fetal compromise prior to the development of significant neurological damage. JOGR. 2014; 40: 2089-2094.
- Maeda K, Nagasawa Automatic computerized diagnosis of fetal sinusoidal heart rate. Fetal Diag Ther. 2005; 20: 328-334.
- Maeda K, Iwabe T, Ito T, et Detailed multigrade evaluation of fetal disorders with the quantified actocardiogram. J Perinat Med. 2009; 37: 392-396.
- Maeda K, Noguchi Y, Nagasawa T, et al. Central computerized automatic fetal heart rate diagnosis with a rapid and direct alarm system. The Open Medical Devices Journal. 2012; 4: 28-33.
- Mizu Fundamental studies on the automatic analysis in fetal heart rate. J JSOG. 1976; 28: 1383-1392.
- Cahill AG, Tuuli MG, Stout MJ, et al. A prospective cohort study of fetal heart rate monitoring: deceleration area is predictive of fetal academia. Amer J Obstet Gynecol. 2018; 218: 523.e1-e12.