Burden, pattern and effects of Rape among women accessing Maternal and Child Health Services in Jos, Nigeria
Author'(s): Stephen A Anzaku1*, Stephen Yohanna2, George I Ogbu3, and Bernard T Utoo4
1Department of Obstetrics and Gynecology, College of Medicine and Health sciences, Bingham University, Jos campus, Nigeria.
2Department of Family Medicine, College of Medicine and Health sciences, Bingham University, Jos campus, Nigeria.
3Department of Obstetrics and Gynecology, Federal Medical Centre, Keffi, Nigeria.
4Department of Obstetrics and Gynecology, College of Health sciences, Benue State University, Makurdi, Nigeria.
*Correspondence:
Anzaku AS, Department of Obstetrics & Gynecology, Bingham University Teaching Hospital, PMB 2238, Jos, Plateau State, Nigeria, Tel: +2348036785049; E-mail: steveanzaku@gmail.com.
Received: 21 June 2018 Accepted: 04 July 2018
Citation: Stephen A Anzaku, Yohanna S, George I Ogbu, et al. Burden, pattern and effects of Rape among women accessing Maternal and Child Health Services in Jos, Nigeria. Gynecol Reprod Health. 2018; 2(4): 1-5.
Abstract
Background: Rape is associated with significant physical, emotional and psychological trauma on the victims and interventions to curb this violent crime among women is a major public health concern. This study aimed at ascertaining the burden, pattern and impacts of rape among women accessing Maternal and Child Health services in Bingham University Teaching Hospital, Jos, Nigeria.
Methods: This was a cross-sectional survey assessing for victims of rape among 251 women recruited by simple random sampling using a pre-tested questionnaire. Inquiries included socio-demographic and obstetric features, history, route, type and place of rape. Other variables sought for included relationship and acquaintance with the perpetrator, number of perpetrators, report of rape as well as any complications following the rape incidence. Data was analyzed using SPSS version 20 (IBM, Armonk, NY, USA).
Results: A total of 39 women reported history of rape, giving a prevalence of 15.5%. Mean age at rape was 19.3 ± 5.9 years with a range of 8–28 years. The commonest routes of rape were through the vagina and anus. Date and acquaintance rape were the commonest, perpetrated by boyfriends in a bedroom. Most of the cases were unreported mostly because of fear of stigmatization and being accused of complicity. Complications faced by the victims were vaginal laceration and bleeding, unwanted pregnancy, anal pain and bleeding, pelvic infections, depression, and lack of trust in men.
Conclusion: Rape is common and often unreported among women in our setting and is associated with immediate and long term complications. Public awareness about rape and its complications as well as the need for reporting of the crime by victims should be implemented so as to eradicate this sexual violence among our women.
Keywords
Introduction
Female sexual violence is a worrisome gender-based violence as well as a public health and human rights problem recognized worldwide [1,2]. Rape which is the extreme version of forced sexual intercourse is often associated with immediate and long term harmful physical, reproductive, psychological and mental consequences, as well as negative impacts on women’s health including chronic pelvic pain and HIV infection [3-6]. Sexual violence may also have tremendous impacts on the social wellbeing of the victims as a result of stigmatization and ostracization by the family members or the society [7].
Rape may be perpetuated by an acquaintance, a stranger, a date or by a spouse within marriage. Estimates of prevalence of rape are limited as a result of differences in methods and definitions used. However, the World Health Organization estimates that globally, every one in five women is a victim of sexual assault [8] but most population based surveys estimated the life time prevalence of rape to be between 10 – 21% among females aged 15 years and above and most cases occur during childhood or adolescence [1,9,10]. About one-third of female adolescents report their first sexual experience as being forced [10-12]. Reports suggest that about 25% of women experience sexual assaults from intimate partners with about two-third suffering rape which is often undisclosed especially if it occurs in marriage setting [10,13]. In Nigeria, 8.8% of women attending gynecological clinic were reported to have been raped in Enugu while 3.6% was reported in Osogbo, South western Nigeria with the rate of rape noted to be increasing [14,15].
Non-disclosure of rape by victims to a third party or law enforcement agencies is a major limitation in the estimation of rape prevalence. Among all forms of sexual violence, rape is the most under-reported crime as only about 39.0% of cases are reported to law enforcement agencies [16]. This is more so when it occurs in marriages and during childhood where most victims do not recognize it as rape [10,13]. Sexual violence occurs worldwide and with increasing prevalence and underreporting of rape, the most severe form of violations of human dignity in the society, this study sought to ascertain the burden, pattern and effects of this sexual violence among women attending Maternal and Child health clinics in Bingham University Teaching Hospital, Jos, Nigeria.
Materials and Methods
This was a descriptive cross-sectional study conducted among women in the Maternal and Child Health service units of Bingham University Teaching Hospital, Jos from July to December 2016. Rape in this context was defined as any unwanted or forced sexual penetration (vaginal, anal or oral) resulting from actual or threatened physical force or when the woman is unable to give affirmative consent. The women irrespective of marital status were recruited by simple random sampling from the immunization clinic, antenatal clinics, gynecological clinics as well as the obstetric and gynecological wards. The women were approached and informed about the study and those that were willing to participate in the study and provided verbal or written consent were included in the sampling population. Women that declined consent and those too sick in the wards were excluded from the study.
A pre-tested questionnaire was used for the study and for women that were literate, the questionnaire was self-administered anonymously and responses filled appropriately. A trained Nurse administered the questionnaires on those that were illiterate and their responses documented. Inquiries made included their socio- demographic and obstetric features as well as intake of alcohol and cigarette smoking. They were also asked about any previous history of forced sexual intercourse and if yes, how many times in their life. Questions were also asked about the number of perpetrators, acquaintance with the perpetrator(s), relationship with the assailant(s), age(s) at time of rape, location of rape, and route of rape. Immediate and late complications developed after the rape, report of the incident and any reason(s) if not reported and the factor(s) that may be responsible for the rape were also ascertained.
A minimum sample size of 246 was calculated using the formula n= Z2Pq/d2 and global estimate of lifetime prevalence of rape and attempted rape of 20.0 [17]. However, with an estimated possible attrition rate of 15%, the number of participants to be recruited was adjusted to 283. Data was analyzed descriptively using SPSS version 20 (IBM, Armonk, NY, USA). Approval for the study was granted by the Human Research and Ethics Committee of Bingham University Teaching Hospital, Jos.
Results
A total of 285 women were recruited and participated in the study but 34 of them filled the questionnaire either incorrectly or incompletely, leaving 251 women whose questionnaires were analyzed. Among the 251 women, 39 (15.5%) reported history of rape in their life. The average age of the entire study population was 31.4 ± 6.2 years with a range of 17 – 45 years while the mean parity was 2.5 ± 1.2. Majority (91.4%) of them were Christians while 8.6% were Muslims.
Among the women with history of rape, the mean age was 29 ± 5.4 years with a range of 18 – 40 years while the mean parity was 1.5 ± 1.3. About 84.6% (33/39) of the women were married while 15.4% (6/39) were single. Thirty seven (94.9%) of them were Christians while two (5.1%) were Muslims. Only 8(20.5%) of them were taking alcohol. Table 1 shows the Socio-demographic and obstetric features of the women with history of rape among the study participants.
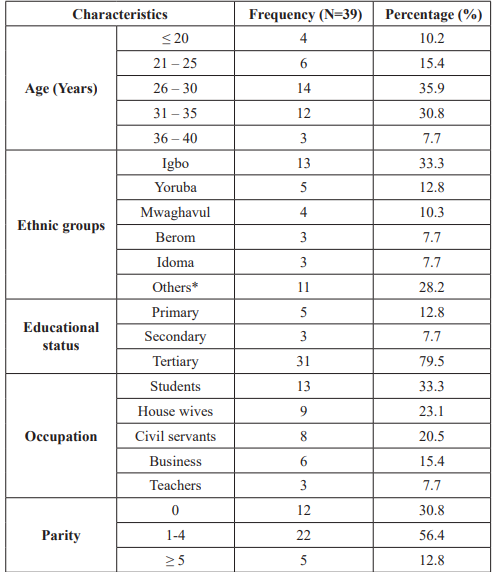
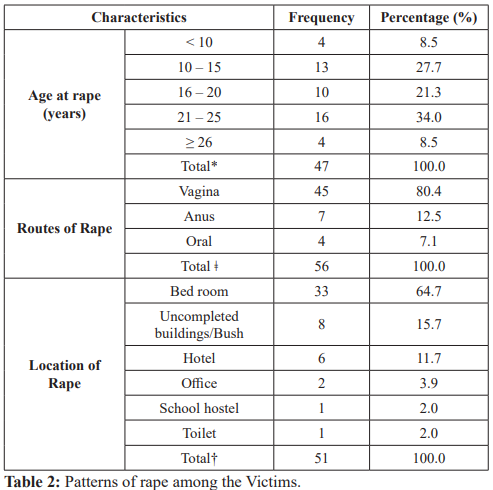
Table 1: Socio-demographic and Obstetric features of women with history of Rape. Others* - Ngas, Irigwe, Kurama, Seyawa, Ijaw, Jenjo, Higgi. As at the time of perpetration of rape, 22 (56.4%) of the victims had multiple sexual partners, 11 (28.2%) had single sexual partners while 6 (15.4%) were not sexually active. However, at the period of the study, majority of the rape victims [37 (94.9%)] had one sexual partner while only 2 (5.1%) had multiple sexual partners. Five (12.8%) women were raped twice or more while 34 (87.2%) were raped once. The mean age at rape was 19.3 ± 5.9 years with a range of 8 – 28 years. Majority of the rape victims [36 (92.3%)] knew the perpetrators while 3 (7.7%) were raped by unknown males (Table 2 depicts the patterns of rape).
*Some women had multiple episodes of rape, Ç? - Some women reported multiple routes of rape †-Some reported multiple locations of rape.
Surprisingly, only 12 (30.8%) of them reported the incident to someone while 27 (69.2%) did not. Six of the women reported the incident to their friends, 3 reported to their mothers while one each reported the rape to their father, Sibling and the law enforcement agency (Police). None of the perpetrators was prosecuted and punished in the court of law. Reasons offered for not disclosing the rape incidents by some of the victims included public stigma as a rape victim [51.9% (14/27), fear of accusation as being responsible for the rape [25.9% (7/27)], threat by the perpetrator [14.8 (4/27)] and felling embarrassed by the act [7.4% (2/27)].
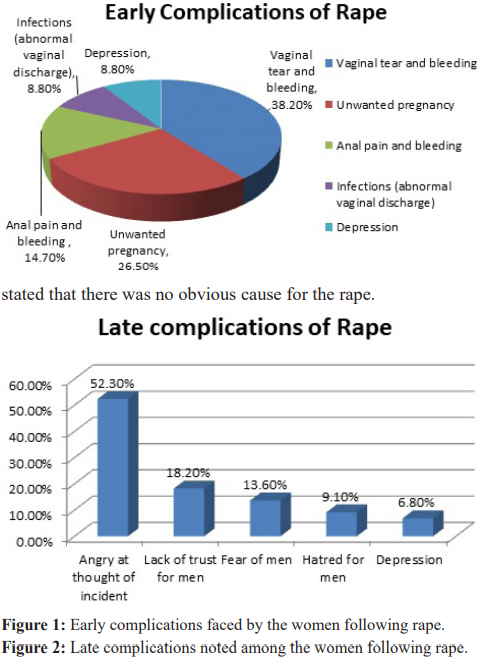
Twenty eight (71.8%) of the victims experienced immediate complications after the rape incidence while 11 (28.2%) did not. However, 36 (92.3%) out of the 39 rape victims believed that they had long term complications including fear and lack of trust for men. Figures 1 and 2 depict the early and late complications faced by the rape victims. When asked about possible contributing factors for the rape incident, the women disclosed that the perpetrator factors including alcoholism, uncontrolled sexual desire, poverty, and drug abuse were responsible while two of the victims believed that their over exposing dressing was responsible. Some however stated that there was no obvious cause for the rape.
Discussion
Sexual violence including rape has tremendous negative impacts on the physical, mental and emotional health of the victims. In this study, 15.5% of the women accessing maternal and child health services (MCH) in this hospital were victims of rape. This is similar to 13.8% rate of sexual assault among female students in Maiduguri and 14.0% among out of school adolescents in a community in Lagos [18,19]. These figures are probably true representation of the occurrence of rape in the general population as our study focused on all women attending MCH units in the hospital. Our reported figure is however higher compared to figures from other regions of Nigeria with prevalence rates of 8.8%, 0.76%, 2.1% and 7.7% among gynecological consultations/ emergencies in Enugu, Lagos, Calabar and Benin respectively [14,20-22]. These differences may be attributable to different study populations and very high denominators of gynecological consultations used in other studies. Prevalence of rape seems to be increasing in the general population [15], and this is also noted in our study compared with a previous reported rate of 5.6% in Jos [23]. This suggests that efforts at tackling this crime in the society must be increased so as to eradicate this human right abuse among women.
Females of all ages face risk of being raped and most cases in the literature occurs among young women as well as Children, adolescents and teenagers [9,10,20-23]. This is similar to the finding in this study and this suggest that awareness about this crime in the populace and education of the girl child on prevention of rape should be commenced early in the school years so as to eliminate this violent crime in the society. Also, enactment of relevant laws on rape and their strict enforcement are essential in halting this sexual violence.
Rape of women has mostly been reported to be through the vaginal route [18-23]. This was also the finding in this study. Additionally, the victims in this study reported that the acts of rape were also perpetrated through the anal and oral routes or combination of these routes. This finding was also reported by other researchers in different populations and settings [24,25].
More than two-third of the victims in this study had date rape while the rest had gang or marital rape. This points to the fact that young women in dating relationships in our environment are more prone of being raped and this is complicated by the fact that there is cultural normalization of sexual coercion in intimate relationships, young women being unaware of date rape and sometimes even victims of date rape do not recognize the act as rape [26,27]. Marital rape has been variously reported in the literature as noted in this study [28,29]. Spousal rape is more or less permitted in our society as women are assumed to be perpetually consented to sexual intercourse in the context of marriage. Hence, married men cannot be held accountable for forced sexual intercourse with their wives and unless this believes is changed through education, this trend may continue.
Majority of the victims of rape in our study knew the assailants (Acquaintance rape) and this is similar to findings globally [21- 26]. However, only few of the victims reported the incident of rape to another individual or law enforcement agencies and this was mainly due to fear of stigmatization, embarrassment and fear of being accused as responsible for the act. This is a reflection of the attitude of the society to victims of rape and unless victims are encouraged to report cases and perpetrators punished appropriately, non-reporting of rape will continue and so indirectly encouraging the crime in the society.
There are diverse health consequences of rape among women. In this study, about three-quarter of the women had immediate complications including vaginal tear and bleeding, anal pain and bleeding, pelvic infections and unwanted pregnancy. This is similar to findings by researchers elsewhere [4-6,20-23,29]. Also, most of the victims believed that the act of rape had long term effects on their emotional and psychological lives including fear and lack of trust in men and depression. These findings underscore the need to eradicate this abnormal behavior especially among the youths as date rape tends to be common.
Many studies reported that many cases of rape are perpetrated by men that are under the influence of alcohol [30,31]and this is was also corroborated by rape victims in this study. Other risk factors for rape identified by the victims included perpetrators’ drug abuse, uncontrolled sexual desire and seductive dressing by some of the women. This again stresses the importance of education of the populace irrespective of gender of the risk factors that contribute to rape.
Conclusion
Rape is relatively common, often unreported and associated with immediate and long term complications on women in our setting. Concerted efforts including public health campaign against this detestable human right violation and its risk factors are required to curb rape and other sexual assaults and their impacts in our society.
Acknowledgement
We sincerely appreciate Mrs. Mary Atu for her immense contribution in distributing the questionnaires to the women as well as administering the questionnaires on some of the subjects.
References
- Garcia-Moreno C, Stockl H. Protection of sexual and reproductive health rights: addressing violence against women. Int J Gynecol Obstet. 2009; 106: 144-147.
- MacDonald Time to talk about rape. BMJ. 2000; 321: 1034-1035.
- Jewkes RK, Dunkle K, Nduna M, et al. Intimate partner violence, relationship power inequity, and incidence of HIV infection in young women in South Africa: a cohort study. Lancet. 2010; 376: 41-48.
- Achunike HC, Kitause Rape epidemic in Nigeria: cases, causes, consequences and responses to the pandemic. IMPACT Int J Res Appl Natl Soc Sci. 2014; 2: 31-44.
- Campbell JC. Health consequences of intimate partner violence. Lancet. 2002; 359: 1331-1336.
- Creamer M, Burgess P, McFarlane Post-traumatic stress disorder: findings from the Australian National Survey of Mental Health and Well-being. Psychological Medicine. 2001; 31: 1237-1247.
- Mollica RF, Son Cultural dimensions in the evaluation and treatment of sexual trauma: an overview. Psychiatric Clinics of North America. 1989; 12: 363-379.
- Garcia-Moreno C, Watts C. Violence against women: an urgent public health Bull World Health Organ. 2011; 89: 2.
- Littleton H, Radecki Breitkopf C, Berenson A. Beyond the campus: unacknowledged rape among low-income women. Violence Against Women. 2008; 14: 269-286.
- Garcia-Moreno C, Jansen HA, Ellsberg M, et al. Prevalence of intimate partner violence: findings from the WHO multi- country study on women's health and domestic violence. Lancet. 2006; 368: 1260-1269.
- Jewkes R, Vundule C, Maforah F, et Relationship dynamics and teenage pregnancy in South Africa. Social science and Medicine. 2001; 52: 733-744.
- Plichta SB, Falik Prevalence of violence and implications for women's health. Womens Health Issues.2001; 11: 244-258.
- McFarlane J. Pregnancy following partner rape - What we know and what we need to Trauma Violence & Abuse. 2007; 8: 127-134.
- Ohayi RS, Ezugwu EC, Chigbu CO, et al. Prevalence and pattern of rape among girls and women attending Enugu State University Teaching Hospital, southeast Nigeria. Int J Gynecol Obstet. 2015; 130: 10-13.
- Adeleke NA, Olowookere AS, Hassan MB, et al. Sexual assault against women at Osogbo, South western Nigeria. Niger J Clin Pract. 2012; 15: 190-193.
- Akinlusi FM, Rabiu AK, Olawepo TA, et al. Sexual assault in Lagos, Nigeria: a five year retrospective review. BMC Women’s Health. 2014; 14: 115.
- MacDonald Time to talk about rape. BMJ. 2000; 321: 1034-1035.
- Kullima AA, Kawuwa MB, Audu BM, et al. Sexual assault against female Nigerian Afr J Reprod Health. 2010; 14: 189-193.
- Kunnuji MON, Esiet Prevalence and Correlates of Sexual abuse among Female Out-of School Adolescents in Iwaya Community, Lagos State, Nigeria. Afr J Reprod Health. 2015; 19: 82-90.
- Akinlusi FM, Rabiu KA, Olawepo TA, et al. Sexual assault in Lagos, Nigeria: a five year retrospective review. BMC Women's Health. 2014; 14: 115.
- Ekabua JE, Agan TU, Iklaki CU, et al. Trauma related to sexual assault in Calabar, South Eastern Niger J Med. 2006; 15: 72-74.
- Akhiwu W, Umanah IN, Olueddo Sexual assaults in Benin City, Nigeria. TAF Prev Med Bull. 2013; 12: 377-382.
- Daru PH, Osagie EO, Pam IC, et Analysis of cases of rape as seen at the Jos University Teaching Hospital, Jos, North Central Nigeria. Niger J Clin Pract. 2011; 14: 47-51.
- Grossin C, Sibille I, Lorin de la Grandmaison G, et Analysis of 418 cases of sexual assault. Forensic Sci Int. 2003; 131: 125-130.
- Riggs N, Houry D, Long G, et al. Analysis of 1,076 cases of sexual assault. Ann Emerg Med. 2000; 35: 358-362.
- Ajuwon AJ, Olley BO, Akinola O, et Sexual coercion in adolescent: exploring the experiences of rape victims in Ibadan, Nigeria. Health Education. 2004; 104: 8-17.
- Oshiname FO, Ogunwale AO, Ajuwon AJ. Knowledge and perceptions of Date Rape among female undergraduates of a Nigerian Afr J Reprod Health. 2013; 17: 137-148.
- Fatusi AO, Alatise OI. Intimate partner violence in Ile-Ife, Nigeria: Women’s experiences and men’s perspectives. Gender Behav. 2006; 4: 764-781.
- Esere MO, Idowu AI, Durosaro IA, et al. Causes and consequences of intimate partner rape and violence: Experiences of victims in Lagos, Nigeria. J AIDS HIV Res. 2009; 1: 1-7.
- Olaleye S, Ajuwon, AJ. Experience of Non-consensual Sex among Students in a Tertiary Institution in Ibadan, Nigeria. Sierra Leone Journal of Biomedical Research. 2011; 3: 175-183.
- Ramisetty-Mikler S, Goebert D, Nishimura S, et al. Dating violence victimization: associated drinking and sexual risk behaviors of Asian, Native Hawaiian, and Caucasian high school students in Hawaii. J Sch Health. 2006; 76: 423-429.