Clinical and Morphological Features of Retrocervical Endometriosis
Author'(s): Almova Indira K1*, Khilkevich Elena G1, Asaturova Alexandra V1, Zaitsev Nikon V1 and Chuprynin Vladimir D2
1National Medical Research Center of Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov, Ministry of Health of Russia, Moscow, Russia.
2Head of the Surgery Department., National Medical Research Center of Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov, Ministry of Health of Russia.
*Correspondence:
Almova Indira K, Postgraduate Student of the Surgical Department, National Medical Research Center of Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov, Ministry of Health of Russia, Moscow, Russia, Tel: +79054357317.
Received: 10 April 2019 Accepted: 06 May 2019
Citation: Almova Indira K, Khilkevich Elena G, Asaturova Alexandra V, et al. Clinical and Morphological Features of Retrocervical Endometriosis. Gynecol Reprod Health. 2019; 3(3): 1-4.
Abstract
Objective: To study the clinical and morphological features in patients with retrocervical endometriosis.
Material and Methods: In National Medical Research Center of Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov, Ministry of Health of Russia, In the period from 2016 to 2018, 120 patients with retrocervical endometriosis were examined and operated on. Patients were divided into 4 subgroups. The extent of retrocervical endometriosis was established according to the gynecological examination (bimanual and rectovaginal examination), ultrasound, MRI, laparoscopy and histological examination of biopsy material.
The Results of the Study: clinical manifestations of retrocervical endometriosis are diverse. High frequency of pain syndrome (pelvic pain, dysmenorrhea, dyspareunia, dyschesia) and infertility in women with external genital endometriosis is an important diagnostic criterion for the disease and determine the indications for laparoscopy. Clinical manifestations of endometriosis, morphologically, can be characterized by in situ factors, oxidative stress, cell roliferation, angiogenesis, destruction and / or proliferation of the nerve ganglia and perineural growth of heterotopies.
Conclusion: patients with RCA need a comprehensive examination, the final stage of which is laparoscopy, removal of all visible endometriotic foci, elimination of adhesive adhesions in the pelvis, followed by morphological study of ectopic foci.
Keywords
Introduction
Deep infiltrative endometriosis is associated with severe pelvic pain and infertility in more than 95% of patients [1] and is accompanied by symptoms such as dysmenorrhea [2], dyspareunia, and in the case of invasion of endometriotic foci into the sacro- uterine ligaments and / or into the wall of the rectum, dyschemia, which has a pronounced negative impact on social life, sexual and psychological well-being, significantly impairing the quality of life [3]. According to numerous studies, asymptomatic disease is observed in 10-22% of the general population [4-6].
Despite the variety of symptoms of retrocervical endometriosis, a correlation is not always observed between the prevalence, the depth of the lesion, the clinical picture and the duration of the disease. The final for the diagnosis of endometriosis remains the intraoperative imaging of endometrioid heterotopies / infiltrates and their histological verification [7].
Objective
To study the clinical and morphological features of patients with external genital (retrocervical) endometriosis.
Material and Research Methods
A comparative analysis of the results of examination and treatment of 120 women of reproductive age, with a histologically verified diagnosis of retrocervical endometriosis received for planned surgical treatment at the National Medical Research Center of Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov, Ministry of Health of Russia (head of department - Mr. VD Chuprynin) in the period from 2016 to 2018.
Depending on the extent of the spread of the pathological process, patients with retrocervical endometriosis are divided into 4 clinical subgroups:
IA subgroup - patients with retrocervical endometriosis without signs of pelvic organ infiltration.
IB subgroup - patients with retrocervical endometriosis and the spread of endometrial infiltration on the wall of the colon.
- IB subgroup - patients with retrocervical endometriosis in combination with endometrial ovarian cysts.
- IG subgroup - patients with retrocervical endometriosis in combination with uterine myoma.
Inclusion criteria
Informed consent to participate in the study, reproductive age, exclusion of hormonal drugs during the last 6 months, histologically confirmed retrocervical endometriosis, absence of oncological diseases and acute inflammatory diseases of the pelvic organs.
Complaints, anamnesis of patients, the menstrual and reproductive functions of patients are studied in detail. All patients underwent laparoscopic surgery under endotracheal anesthesia according to the standard procedure in the Trendelenburg position. The volume of surgical treatment in patients with external genital endometriosis included excision of endometrial foci within visually healthy tissues, followed by pathological examination of the removed material. As shown in Table 1, all patients with NGE were dissected foci of retrocervical endometriosis (n = 120), in an equal number of patients in four subgroups (n = 30) - resection of the ovaries was performed, the intestines, for infiltrative growth, also in some patients in combination with uterine myoma performed enucleation of myomatous nodes during surgery.
Histological examination
Macroscopic evaluation of the removed macropreparation was carried out, then fixed in 10% neutral formalin solution for 24 hours and according to the standard protocol of histological tissue placement, embedded in paraffin. After staining the sections with hematoxylin and eosin, a further morphological study was performed according to the standard standard technique. Pathological examination was carried out in the pathoanatomical department of the National Medical Research Center of Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov, Ministry of Health of Russia.
Research Results
120 patients aged 21 to 45 years were examined, the average age was 33.75 ± 5.25 years. The main complaints of patients of the IA subgroup during hospitalization were: the absence of pregnancy from 1 to 2 years in 26 (86.7%) patients, pulling pain in the lower sections of the stomach of a periodic nature in 29 (96.6%) (p> 0.05).
Complaints of pain in the lower abdomen with irradiation in the perineum indicated 9 (30%), sacral area 14 (46.7%), in the lower extremities 7 (23.3%) women IB subgroups (p> 0.05).
In patients of subgroup IB with infiltrative endometriosis growing into the colon wall, the main complaints during hospitalization were: pain during sexual contact in 16 (53.3%) women, bleeding from the rectum during menstruation in 8 (26.6%) patients (p> 0.05) in combination with a significant deterioration in general well-being. When detailing complaints, subgroup IB patients also noted abdominal distention before and during menstruation (18 (60%) women), weakened stools (12 (40%) patients (p <0.05). Diarrhea alternated with frequent constipation outside menstruation, in this connection, patients repeatedly turned to a surgeon, coloproctologist, and gastroenterologist.
In patients with retrocervical endometriosis and uterine myoma - IG subgroups, a combination of symptoms such as heavy menstruation (20 (66.6%) women), "bloody" brown discharge from the genital tract before and after menstruation for 5 days (9 (30%) patients), nagging pain in the lower abdomen of a periodic nature (12 (40%) patients) were the main complaints during hospitalization (p> 0.05).
All patients characterized the pain syndrome as a complex manifestation of the disease in combination with weakness, sleep disturbance, reduced working capacity, and a depressive state.
One of the main complaints in patients was dyspareunia, which was mainly observed in 22 (73.3%) patients in the IB subgroup and in 17 (56.6%) (p<0.05) in the IA subgroups.
The average duration of the menstrual cycle in the studied subgroups was 28.71 ± 5.10 days. The longest menstrual bleeding was observed in subgroups IB and IG, which was 7.67 ± 2.12 days (p = 0.02). In assessments of variability by volume of menstrual bleeding, both in the IA and IB and IG subgroups, that is, in 24 (80%), 18 (80%), 21 (70%), respectively, patients were assessed as moderate and 25 (83.3%) IG subgroups are abundant (p = 0.02).
When evaluating the reproductive function of patients with different manifestations of the underlying disease, statistically significant differences were noted only in the number of births, the largest number of births in patients of the IA subgroup was in 17 cases (60.7%), the smallest number of births in the IB subgroup were in 13 patients (48 , 2%) (p <0.05).
Morphological study
Macroscopically, foci of retrocervical endometriosis were tissue fragments ranging in size from 0.2 to 3.0 cm, fibrous structure, with an uneven surface, the presence of punctate cystic cavities. Endometrioid ovarian cysts were cystic cavities with thickened fibrous walls, a smooth outer surface and a folded inner one, with brown overlays, measuring from 1.0 to 5.0 cm (Figure 1b). Remote infiltration of the intestine was presented in the form of areas of the intestine with an unevenly thickened wall due to hypertrophy of muscle fibers and deformation and / or narrowing of the lumen of the intestine of varying severity. In the area of the lesion on the mucous membrane of the intestine smoothing of internal folds was noted. Myomatous nodes were characterized by fibrous tissue of a whitish color, dense structure, fibrous structure, sizes from 1.0 to 8.0 cm (Figure 1a).
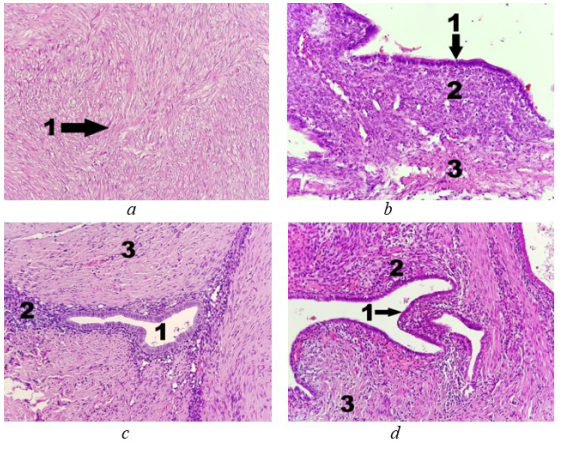
Figure 1: Microscopic characteristics: a - Fragment of uterus myomatous node: 1 - bundles of leiomyocytes; b- Fragment of an endometrioid ovarian cyst: 1 - endometrial epithelium; 2 - endometrial stroma; 3 - ovarian stroma; c - Fragment of the endometrial focus of the upper ampullary colon: 1 - lumen of the endometrial gland; 2 - endometrial stroma; 3 - the muscular layer of the intestinal wall; d - Fragment of retrocervical endometriosis: 1 - endometrial epithelium; 2 - endometrial stroma; 3 - connective tissue. Eyepiece 10x. Lens 20x. Stained with hematoxylin and eosin.
Microscopically, foci of endometriosis were characterized by fibrous-muscular tissue with a fatty component. An analysis of the characteristics of endometriotic foci of retrocervical fiber showed that endometrioid heterotopies are represented by a glandular and stromal component, with a different combination of the so-called “active” and “inactive” heterotopies (Figure 1d). Active foci were characterized by pronounced vascularization, cytogenic stroma and glands lined with proliferating type epithelium. Inactive - moderately severe, mostly sclerotic cytogenic stroma, with deformed glands cystic-expanded, lined by atrophic or dystrophic modified epithelium. Outbreaks of retrocervical endometriosis contain a more pronounced stromal component, while in the foci of ovarian endometriosis a glandular component predominated, with a minimal constituent stromal component. The glandular component can be represented by a flattened epithelium and / or cystic extended gland with a slit-like or rounded lumen, proliferating, secretory (rarely), or indifferent epithelium. In some places, the stromal component of heterotopia had the appearance of an “active” one, rich in inflammatory cells and sinusoidal vessels, and in some places sclerotic cells. It was found that the foci had a cytogenic stroma and areas of fibrous muscular tissue that were infiltrated with inflammatory cells - lymphocytes, macrophages, eosinophils, and to a lesser extent, neurophilic leukocytes, which is characteristic of chronic inflammation, often in the phase of exacerbation. In all subgroups, the deformation of the surrounding tissues with foci of sclerosis, hemorrhages of various periods, accumulation of hemosiderin and inflammatory reaction were noted. The hypertrophy of muscle fibers localized around the endometriotic foci imitated the architectural features of the myometrium.
The most “aggressive” (proliferatively active, rich in stromal component) foci were found in patients with retrocervical endometriosis spreading on the intestinal wall. Foci were represented by cystic-modified endometrial glands with surrounding cytogenic stroma in fibro-adipose tissue with hypertrophy of the surrounding smooth muscle tissue (Figure 1c). Foci were characterized by proliferative activity, mainly with perivascular and perineural growth. In the IG subgroup, all endometrial foci had low proliferative activity, without intravascular growth. In the foci of endometriosis IB subgroups were found invasion of endometrioid heterotopias in the nerve terminals, lymphatic and blood vessels. Connective tissue growths were detected around endometrioid heterotopies with lymphocytic and macrophage infiltration, hemosiderin accumulation, angiomatosis foci, deformed and hypertrophied nerve fibers. A large number of neutrophils, eosinophils, mast cells and lymphomacrophagal infiltration were detected around heterotopias. In the adjacent muscle tissue, pronounced hypertrophy of smooth muscle cells with perifocal inflammation was detected. It was noted the growth of nerve endings with the destruction of fibers in the form of randomly located conglomerates.
In the scraping from the uterus in the secretion phase in patients with RCA, the endometrium was presented with a mucous membrane with convoluted glands and a wide lumen, the epithelium of the glands is multi-row, with signs of secretion into the lumen of the glands, stroma with edema, vascular thickening with the formation of coils of spiral arteries. In the proliferation stage, endometrial fragments were characterized by the presence of tubular glands lined with a single-row epithelium of proliferative type, with the presence of mitoses and apoptotic bodies, cytogenous stroma with diffuse lymphoid infiltration.
Thus, infiltrative growth of endometriosis can be observed in the intermuscular spaces, glial sheaths of nerve fibers, ganglia, along the vessels of the microcirculation system and lymph nodes. Infiltration of nerve endings with endometriosis leads to damage to the nerve fibers and nodes with impaired regenerative abilities and the formation of neurinomas. Perivascular fibrosis leads to stagnation in the capillary network and lymphostasis, which increases the oxidative stress and inflammatory response of the cell.
Discussion
Analysis of anamnestic and clinical data revealed a number of features characteristic of infiltrative endometriosis. According to the literature, severe forms of external genital endometriosis occur mainly in women of late reproductive age [8]. However, our results do not agree with the literature data, which indicate a correlation of infiltrative forms of endometriosis with an increase in the age of patients. In the present work, the average age of patients with infiltrative forms of external genital endometriosis was 33.75 ± 5.25 years, which corresponds to the reproductive age and may indicate the possibility of further progression of the disease.
It should be noted that in the clinical picture of the disease, pain syndrome is a classic symptom and the main problem that worsens the quality of life of patients, which corresponds to the results of domestic and foreign researchers [9-11].
In women with retrocervical endometriosis germination, predominantly “active and aggressive” foci of endometriosis prevailed in the intestinal wall, represented by proliferating and hyperplastic epithelium with cytogenic stroma and glands, as well as intravascular and perineural growth of foci. Thus, endometriosis grows into anatomical structures and organs, with gradual damage to the vascular networks and nerve endings, which is characterized by a long sluggish process and features of clinical manifestations. Among the fields of sclerosis in the foci of endometriosis, deformed, hypertrophied nerve fibers and blood micro vessels were identified, sometimes forming conglomerates. In some cases, a concentric arrangement of the nerve ganglia along the periphery of endometrial foci with signs of fiber destruction was observed. These changes lead to the release of chemically active agents, the development of an inflammatory reaction, which results in the release of inflammatory mediators - cytokines, which is consistent with the data of several researchers [12,13]. These substances lead to a high sensitivity of nerve endings, as a result of which a pain signal is formed.
All this allows to partially answer the question - why not all women have a pronounced clinical picture. It is possible that ectopic tissue has universal molecular biological properties; it organizes around itself immune response cells that promote proliferating, adhesive, invasive, implantation properties of eutopic endometrium.
Conclusion
Thus, women with retrocervical endometriosis are characterized by a severe form of the disease with a tendency to infiltrative growth of foci, damage to adjacent organs, nerve plexuses and blood microvessels.
Invasive activity and dissemination of the process with the formation of deep infiltrative foci in RCA is due to the increased expression of vasoactive molecules, growth factors in eutopic and ectopic endometria, which reaches a maximum during germination of retrocervical endometriosis in the intestinal wall.
The given clinical and morphological results indicate that Laparoscopy remains the main criterion for the treatment and diagnosis of endometriosis, followed by a morphological study of endometriosis foci.
References
- Koninckx PR, Ussia A, Adamyan L, et Deep endometriosis: definition, diagnosis, and treatment. Fertil Steril. 2012; 98: 564-571.
- Federal clinical guidelines for the management of patients. Endometriosis: diagnosis, treatment and rehabilitation. 2013; 1-70.
- Tikhonchuk EYu, Asaturova AV, Adamyan LV. Molecular biological changes of the endometrium in women with external genital endometriosis. Obstetrics and gynecology. 2016; 11: 42-48.
- Vercellini P, Somigliana E, Consonni D, et al. Surgical Koninckx versus medical treatment for endometriosis- associated severe deep dyspareunia: I Effect on pain during intercourse and patient satisfaction. 2012; 27: 3450-3459.
- Menakaya U, Reid S, Lu C, et Performance of ultrasound- based endometriosis staging system (UBESS) for predicting level of complexity of laparoscopic surgery for endometriosis. Ultrasound in obstetrics & gynecology. 2016; 48: 786-795.
- Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertility and Sterility. 2012; 98: 511-519.
- Vercellini P, Somigliana E, Viganò P, et al. Post-operative endometriosis recurrence: a plea for prevention based on pathogenetic, epidemiological and clinical evidence. Reprod Biomed Online. 2010; 21: 259-265.
- Gordts S, Koninckx P, Brosens I. Pathogenesis of deep endometriosis. Fertil Steril. 2017; 108: 872-885.
- Ozawa Y, Murakami T, Terada Y, et al. Management of the pain associated with endometriosis: an update of the painful problems. Tohoku J Exp Med. 2006; 210: 175-188.
- Howard FM. Endometriosis and mechanisms of pelvic pain. Invasive Gynecol. 2009; 16: 540-606.
- Momoeda M, Taketani Y, Terakawa N, et Is endometriosis really associated with pain? Gen Obstet Invest. 2002; 54: 18- 23.
- Akoum A, Al-Akoum M, Lemay A, et al. Imbalance in peritoneal levels of interleukin 1 and its decoy inhibitory receptor type II in endometriosis women with infertility and pelvic pain. Fertil Steril. 2008; 89: 1618-1624.
- Yorie Ohata, Tasuku Harada, Hiroko Miyakoda, et al. Serum interleukin-8 levels are elevated in patients with ovarian endometrioma. Fertil Steril. 2008; 90: 994- 999.