Drospirenone Containing Combined Oral Contraceptive Premedication before Letrozole Ovulation Induction in Clomiphene Resistant PCOS, Is it Worth the Wait?
Author'(s): Mohamed Salama MD and Haitham Hamza MD*
Department of Obstetrics and Gynecology, Faculty of Medicine, Menoufia University, Menoufia governorate, Egypt.
*Correspondence:
Haitham Hamza, Department of Obstetrics and Gynecology, Faculty of Medicine, Menoufia University, Menoufia governorate, Egypt, Tel: +201001359136.
Received: 29 March 2019 Accepted: 24 April 2019
Citation: Mohamed Salama, Haitham Hamza. Drospirenone Containing Combined Oral Contraceptive Premedication before Letrozole Ovulation Induction in Clomiphene Resistant PCOS, Is it Worth the Wait?. Gynecol Reprod Health. 2019; 3(2): 1-6.
Abstract
Objective: This prospective randomized study aimed to study whether pretreatment with drosperinone containing COC before letrozole induction of ovulation could improve the response in clomiphene (CC)-resistant women with polycystic ovarian syndrome (PCOS).
Methods: The study comprised a total of 125 infertile women (227 cycles) with CC resistant PCOS selected from the clinics affiliated to the Department of Obstetrics and Gynecology of Menoufia University - Egypt. Patients were randomized to either group (A) (61 patients, 116 cycles), patients received drospirenone-containing oral contraceptive pills (OCP) for 42 days then letrozole 2.5 mg twice daily starting from the 2nd day of menstruation for 5 days and group (B) patients received letrozole in the same manner but without OCP pretreatment (64 patients, 111 cycles). 10000 IU hCG administered when mature follicles reached ≥ 18 mm in diameter. Data obtained were statistically analyzed using SPSS software version 20 for Windows. Unpaired t-test used to compare means between both groups while paired t-test used to compare means in group A before and after COC pretreatment, proportions were analyzed using the χ2 test, correlations were analyzed with Pearson correlation and logistic regression and ROC curve used for analysis of the predictors for pregnancy in group (A). A P value of less than .05 was considered statistically significant.
Trial ID: PACTR201611001569368.
Results: Ovulation was significantly higher in Group (A) than in group (B) 98/116 cycles (84.5%) and 74/111 cycle (66.7 %), p=0.003, clinical pregnancy rate was significantly higher in Group (A) than in group (B)32/116 cycles (27.6%) and 16/111 cycle (14.4%), p=0.02. Statistically significant decrease in LH (14.9 ± 3.96 vs 6.8 ± 2.6), Testosterone (2.2 ± 0.72 vs 1.2 ± 0.68) and FAI (8.9 ± 2.3 vs 4.1 ± 1.8) and DHEAS (254.0 ± 92.49 vs 165.8 ± 48.79) and increase in SHBG (25.4 ± 13.67 vs 56.5 ± 12.95) and ovarian stromal pulsatility index “OSPI” (0.9 ± 0.07vs 1.06 ± 0.06) were observed in group (A) before and after pretreatment with COC (p value < 0.001). There were no significant changes in BMI, FSH, fasting insulin and glucose and HOMA-IR. After OCP pretreatment, the mean change in LH correlated positively with the mean change in testosterone and free androgen index “FAI” (p=0.006 and 0.013 respectively) and the mean change in ovarian stromal pulsatility index (OSPI) correlated negatively with LH, testosterone and FAI (p=0.02, 0.007 and 0.013 respectively). The best predictors for pregnancy in group (A) were change in LH, testosterone and FAI at cutoff points (≤ -7.72 mIU/ml, ≤ -1.04 nmol/ml and ≤ -5.02respectively) with sensitivity /specificity (91.2/74.07, 82.4/88.9 and 79.4/85.2 respectively).
Conclusion: Pretreatment with drospirenone-containing COC before letrozole ovulation induction in patients with CC-resistant PCOS can improve ovulation and pregnancy rates.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrine disorder among women that is characterized by chronic anovulation presenting with up to 30% of infertility in couples seeking treatment [1]. Clomiphene citrate (CC) is still the standard drug for inducing ovulation however 15-20% of patients don’t ovulate with CC induction (CC resistance “CCR”) [2]. Aromatase inhibitors (AIs) and gonadotropins are the most common alternative therapies to induce ovulation in CCR patients. The drawbacks of gonadotropin therapy are being expensive, risk of high-order multiple gestations and ovarian hyperstimulation syndrome [2]. Letrozole is a potent, reversible, and highly selective AI that prevents androgen-to-estrogen conversion, it increases follicle stimulating hormone (FSH) by decreasing the negative feedback of estrogens in the hypothalamus. Letrozole is considered ideal for ovulation induction, as it does not decrease estrogen receptors in target tissues with less negative impact on endometrium and cervical mucus, and it typically favoring mono-follicular growth [3]. Previous studies showed that the use of oral contraceptive pills (OCP) for 2 months in CCR women before repeating CC induction of ovulation produced effective ovulation and pregnancy rates. It was suggested that this approach may avoid the high cost and risks of gonadotropin therapy [4]. Several studies showed that drospirenone-containing OCPs may be more effective in the treatment of PCOS than the traditional OCPs [5].
This study was designed to evaluate the effectiveness of 42 days of drospirenone-ethinyl estradiol OCP pretreatment followed by letrozole induction of ovulation in patients with CCR.
Materials and Methods
This was a randomized controlled study carried out at the department of Obstetrics and Gynecology, faculty of Medicine, Menoufia university, Shibin El-kom, Menoufia, Egypt, during the period between September 2016 and March 2018. The study protocol was reviewed and approved by the local review board and the ethical committee at faculty of Medicine, Menoufia university, an informed consent has been taken from all patients before starting the study. The sample size was calculated using Med Calc Statistical Software version 14.8.1 (MedCalc Software bvba, Ostend, Belgium) based on an expected rate of ovulation of 59 % in the letrozole group [6] a total of 116 women were required to show an absolute increase of 25% in ovulation rate in the pretreatment group, with a power of 80%. One hundred and twenty-five patients diagnosed with PCOS according to the revised Rotterdam criteria, who failed to respond to CC 150mg daily for five days after 3-6 cycles of stimulation [2] were recruited. Other criteria for inclusion in the study were; a normal semen analysis, normal uterus, and patent both tubes. Exclusion criteria were; endocrine disorders as hyperprolactinemia, thyroid, and adrenal gland diseases and anatomic abnormalities as uterine fibroids, endometriosis, ovarian cyst, and pelvic inflammatory disease.
After thorough evaluation and investigations, 125 patients were enrolled (Figure 1). Randomization was carried out using computer generated simple random tables with patients allocated into one of the two groups: group A (61 patients, 116 cycles), patients assigned to receive combined oral contraceptive pills containing 3mg drospirenone and 30µg ethinyl estradiol (Yasmin, Bayer Schering, Germany) for 42 days then letrozole (Letrozole 2.5mg, Acdima International, Egypt) 2.5 mg twice daily starting from the second day of menstruation for 5 days and group (B) (64 patients, 116 cycles) patients assigned to receive 2.5 mg twice daily starting from the second day of menstruation for 5 days without OCP pretreatment.

Figure 1: CONSORT flow diagram.
Biochemical assays
An early-morning blood sample was obtained during the follicular phase (day 3 of the spontaneous cycle or progestin-induced menses in case of amenorrhea) for the measurement of follicle stimulating hormone (FSH), luteinizing hormone (LH), total testosterone (T), sex hormone binding globulin (SHBG), dehydroepiandrosterone sulfate (DHEAS), insulin, and glucose. Six milliliters blood samples drawn from each patient and collected in vacutainer tubes. All samples were then centrifuged 2 hours after withdrawal and were stored at −20°C until assayed. FSH, LH, insulin, T, and DHEAS were measured using an enzyme immunoassay (DRG Instruments, Marburg, Germany). SHBG concentrations were measured in serum by an immunoradiometric assay (IRMA, Immunotechs.r.o.). Fasting blood glucose was measured on an automated autoanalyzer (Roche Diagnostics GmbH, Mannheim, Germany).IR was calculated using the Homeostasis Model Assessment (HOMA) index as follows: HOMA-IR = fasting insulin (μIU/ml) × fasting glucose (mg/dl) / 405.
Doppler study for ovarian stromal pulsatility index (OSPI) All patients were studied between 8:00a.m. and 11:00a.m. to exclude the effects of the circadian rhythm on ovarian blood flows. Ultrasound was performed after 15 minutes rest with the urinary bladder empty using transvaginal probe of Voluson S6 machine (GE Medical Systems, Milwaukee, WI, USA). Stromal blood vessels were sought by means of color and power doppler. If more than one blood vessel detected, the vessel with the lowest resistance only was chosen for analysis. Mean values for PIs of the left and right ovaries were calculated and recorded.
Follow up In both groups, folliculometry was started on day 7 till administration of human chorionic gonadotrophin (hCG) (Epifasi 5000IU, ampoule, EIPICO pharmaceuticals, Egypt) and confirmation of ovulation by ultrasound (fluid in the cul-de-sac, and/or echogenic cyst consistent with corpus luteum) and midluteal progesterone >3 ng/dl. Pregnancy was confirmed by serum hCG levels and fetal cardiac activity by transvaginal ultrasound scan. Follicle growth, endometrial development, and pregnancy rate were recorded for each patient and treatment cycle. In case of ovulation in the initial cycle without pregnancy, letrozole induction was repeated in the same dose next cycle and follow up was the same as described before. This process was repeated for a maximum of 3 cycles.
Outcome measures
Ovulation rate, endometrial thickness at time of hCG administration and pregnancy rate during the three cycles of stimulation.
Statistical analysis
Data obtained were statistically analyzed using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL) software version 20 for Windows. Unpaired t-test used to compare means between both groups while paired t-test used to compare means in group A before and after COC pretreatment, proportions were analyzed using the χ2 test. The correlations were analyzed with Pearson correlation. Logistic regression and ROC curve used for analysis of the predictors for pregnancy in group (A). P value of less than .05 was considered statistically significant and <.001 was highly significant.
Results
Table 1 depicts patients’ characteristics. There were no statistically significant differences between both groups regarding age, body mass index, infertility duration, baseline hormonal profile and ovarian stromal pulsatility index (OSPI) (p>.05). Comparison regarding BMI, hormonal profile and OSPI in group (A) before and after pretreatment with OCP is shown in Table 2. LH, testosterone, FAI and DHEAS were significantly lower after OCP pretreatment (p<.001). While SHBG and OSPI were significantly higher after OCP pretreatment (p<.001). Table 3 shows comparison between group (A) and (B) regarding cycle outcomes. Ovulation was significantly higher in group (A) than in group (B) (p=0.003), Pregnancy rate per patients and cumulative pregnancy rate per cycles were significantly higher in group (A) than in group (B) (p=0.003 and 0.02 respectively).
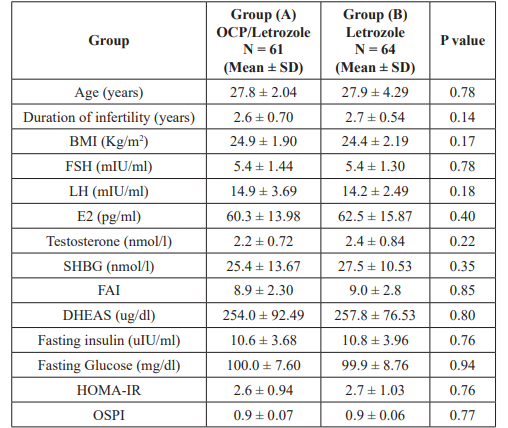
Table 1: Comparison of the baseline parameters between the two study groups.
OCP: Oral Contraceptive Pills; BMI: Body Mass Index; FSH: Follicle Stimulating Hormone; LH: Luteinizing Hormone; E2: Estradiol; SHBG: Sex Hormone Binding Globulin; FAI: Free Androgen Index; DHEAS: Dehydroepiandrosterone Sulfate; HOMA-IR: Homeostasis Model of Insulin Resistance; OSPI: Ovarian Stromal Pulsitility Index.
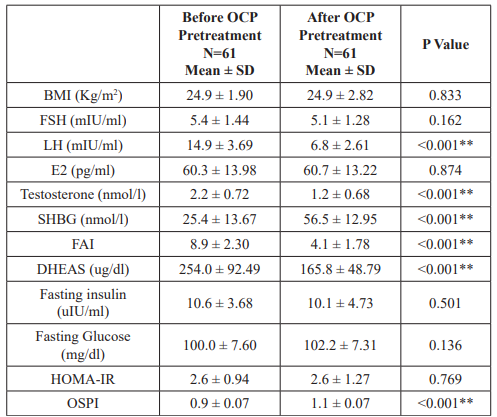
Table 2: Comparison of clinical, biochemical and Doppler values before and 42 days after OCP pretreatment in group (A).
** Highly significant. Footnotes as Table 1.
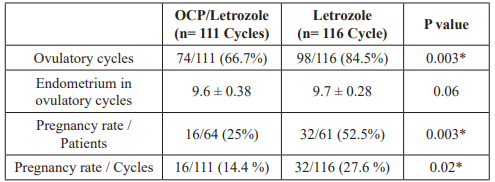
Table 3: Comparison between group (A) and group (B) regarding cycle outcomes.
* Significant. OCP: Oral Contraceptive Pills.
Figures 2A, 2B and 2C show correlations significant negative correlation between mean change in OSPI and mean change in LH, testosterone and FAI (p=0.02, 0.007 and 0.013 respectively) while figures 2D and 2E show a significant positive correlation between mean change in LH and FAI and testosterone (p= 0.006 and 0.013 respectively). Table 4 depicts logestic regression analysis for predictors of pregnancy in group A. The mean change in LH, testosterone and FAI after OCP pretreatment were the best predictors of pregnancy in group (A) (p= 0.011, 0.017 and 0.019 respectively). Table 5 and Figure 3 shows ROC curve analysis for predictors of pregnancy in group (A).
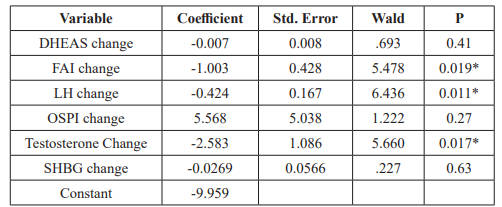
Table 4: Logistic regression analysis for predictors of pregnancy in group
(A). * Significant. Footnotes as table 1.
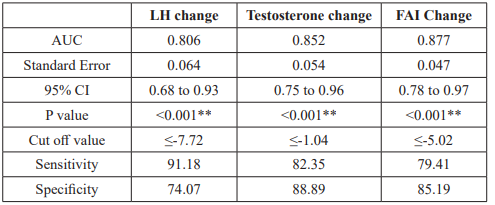
Table 5: ROC curve analysis for predictors of pregnancy in group (A).
**Highly significant. LH: Luteinizing Hormone; FAI: Free Androgen Index; AUC: Area Under ROC Curve; CI: Confidence Interval.
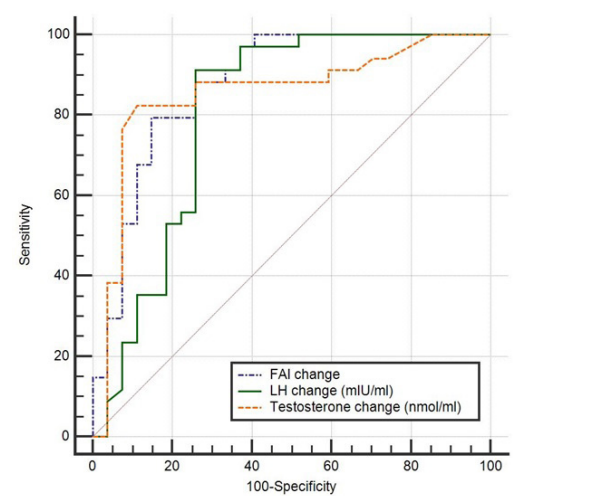
Figure 3: ROC curves for best predictors of pregnancy in group (A). FAI: Free androgen index; LH: Luteinizing hormone.
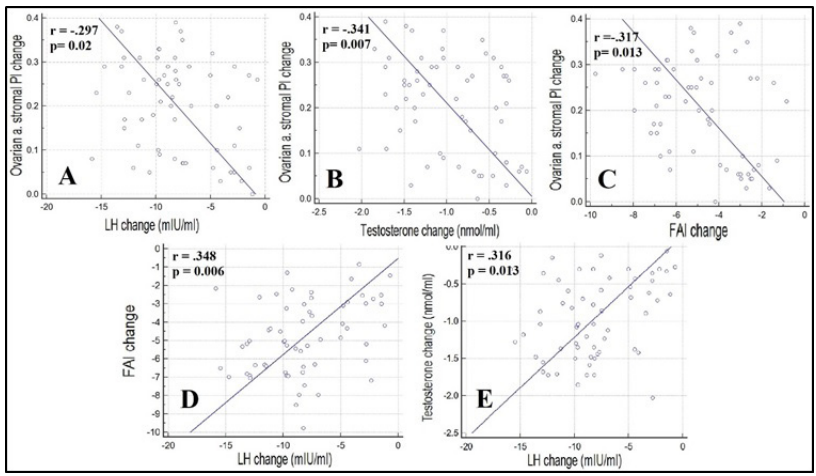
Figure 2: Correlations between change in ovarian stromal PI and change in Luteinizing Hormone “LH” (A), Testosterone (B) and Free androgen index “FAI” (C) and correlation between change in LH and change in FAI (D) and change in Testosterone (E).
Discussion
Several studies investigated the response to CC in PCOS patients and several biochemical, mainly high LH and androgen levels, and ultrasonographic markers have been proposed as predictors of CC resistance [7]. For the last few years, letrozole took the lead for ovulation induction for CC-resistant PCOS either alone or combined with metformin or gonadotrophins [3].
The idea of the current study was to answer the question; if letrozole proved effective to induce ovulation and provide satisfactory pregnancy rates in CCR patients, can we maximize these responses if we manipulated the factors that were proposed to be responsible for the CC resistance in the first place?
This concept was first introduced by Branigan and Estes in 2003, they could achieve ovulation and pregnancy using CC in patients that were CC-resistant, only after 42 day of ovarian suppression by desogestrel-containing OCPs and they attributed this to the significant reduction in LH and androgen levels.
In the current study, pretreatment with drospirenone containing oral contraception for 42 days in patients with CC-resistant PCOS was associated with a statistically significant reduction in LH serum levels whereas no significant changes were found in FSH levels. In agreement with this work, Branigan and Estes conducted a randomized controlled trial on patients with CC resistant anovulation with the use of contraceptive pill suppression and repeat clomiphene citrate induction. After 42-50 days of pill suppression, patients showed significant reduction in LH levels while no effect noted on the FSH levels [4]. Okyay et al. found that after 3 months of OCP treatment for patients with PCOS there was marked decrease in LH levels, however, in contrast to the current study, they also found a decrease in FSH levels [8]. This may be attributed to the longer duration of 3 months in their study rather than the 42 days pretreatment in this study, also the population of this study includes only CCR patients.
Regarding androgen levels, the current study demonstrated a significant decrease in DHEAS, total Testosterone and FAI and a significant increase in SHBG after 42 days of OCP pretreatment. De Leo et al.in their study of the effect of oral contraceptives on markers of hyperandrogenism and levels of SHBG in PCOS patients found similar results, they concluded that oral contraceptives particularly those containing antiandrogenic progestogens as drospirenone proved more effective in counteracting the high androgen levels in those patients [9]. Suvarna et al.in a study that aimed to compare metformin versus ethinylestradiol/drospirenone OCP in PCOS they noted that after 3 months of OCP use there were significant reduction in DHEAS and testosterone levels [10]. These results are in line with the earlier studies that investigated the use of drospirenone-containing OCP in the treatment of PCOS. Guido et al. also found that SHBG rises early after use of drospirenone-containing OCP, is long-lasting and was greater than that found with 17α-hydroxyprogesterone containing OCP. They thus concluded that drospirenone-containing OCPs is better than for treatment of PCOS associated hyperandrogenemia [11-13]. A recently published meta-analysis by Amiri et al notices a decrease in Testosterone and increase in SHBG but no change in FSH and LH in PCOS patients after 3 months of use of drospirenone containing OCPs, 3 months more of use results in a significant decrease in LH and FSH levels. Difference from our results could be attributed to the continuous use of the OCP in our study rather than the regular use of the OCP in the meta-analysis [14]. Noteworthy in the current study, the mean change in LH after OCP pretreatment was significantly correlated to the mean change in testosterone and FAI (i.e. the more the LH decreases after OCP treatment the more the decrease in testosterone and FAI).
As drospirenone is less androgenic, it appears that the metabolic effects that develop with other OCPs are lower or even absent in PCOS patients using drospirenone-containing OCPs [5]. Previous studies demonstrated no change in fasting glucose, fasting insulin and HOMA-IR in PCOS patients using drospirenone containing OCPS [8,15,16]. Similarly, in the current study there were no significant changes in these parameters in CC-resistant PCOS after 42 days of OCP pretreatment.
Increased stromal vascularization has been shown to be prominent in polycystic ovaries particularly in CCR patients [7]. In 2015, Ozdemir et al. linked this to new angiogenesis resulting from hyperplasia of ovarian theca/stromal cells secondary to elevation of LH and LH/FSH ratios [17]. Amin et al. found that the increase in LH levels was correlated with vascular endothelial growth factor (VEGF) and insulin-like growth factor-1 (IGF-1). VEGF and IGF- 1 play a role in neoangiogenesis which lead to increased stromal vascularization in PCOS [18]. After 42 days of OCPs pretreatment current study shows significant increase in the OSPI which is consistent with the findings of Okyay et al. [8]. Interestingly, in this study it was also found that there are significant negative correlations between the change in LH, testosterone and FAI and OSPI i.e. the more the decrease in LH, testosterone and FAI after OCP treatment the higher the degree of increase in OSPI. These findings may highlight the underlying etiology of increased ovarian blood flow in CC-resistant PCOS.
To the best of our knowledge it is the first study to compare the Letrozole induction of ovulation with and without a 42 days pretreatment period with drospirenone containing OCP. In this study, pretreatment with OCPs was associated with higher rates of ovulation, no change in endometrial thickness and higher clinical pregnancy rates in CC resistant patients compared to patients who didn’t receive pretreatment. In patients who received pretreatment, mean changes in levels of LH, Testosterone and FAI from baseline were the best predictors of pregnancy.
Large multicenter studies are required to confirm or refute our findings.
References
- Vitek W, Hoeger K, Legro RS. Treatment strategies for infertile women with polycystic ovary syndrome. Minerva Ginecol. 2016; 68: 450-457.
- Palomba S, Falbo A, Zullo F. Management strategies for ovulation induction in women with polycystic ovary syndrome and known clomifene citrate resistance. Curr Opin Obstet Gynecol. 2009; 21: 465-473.
- Franik S, Eltrop SM, Kremer JA, et al. Aromatase inhibitors (letrozole) for subfertile women with polycystic ovary syndrome. Cochrane Database Syst 2018; 5: Cd010287.
- Branigan EF, Estes MA. A randomized clinical trial of treatment of clomiphene citrate-resistant anovulation with the use of oral contraceptive pill suppression and repeat clomiphene citrate treatment. Am J Obstet Gynecol. 2003; 188: 1424-1428.
- Ruchi Mathur, Olga Levin, Ricardo Azziz. Use of ethinylestradiol/drospirenone combination in patients with the polycystic ovary Ther Clin Risk Manag. 2008; 4: 487-492.
- Abdellah MS. Reproductive outcome after letrozole versus laparoscopic ovarian drilling for clomiphene-resistant polycystic ovary Int J Gynaecol Obstet. 2011; 113: 218-221.
- Ellakwa HE, Sanad ZF, Hamza HA, et Predictors of patient responses to ovulation induction with clomiphene citrate in patients with polycystic ovary syndrome experiencing infertility. Int J Gynaecol Obstet. 2016; 133: 59-63.
- Okyay E, Gode F, Acet F, et The effect of drospirenone (3 mg) with ethinyl estradiol (30 mcg) containing pills on ovarian blood flows in women with polycystic ovary syndrome: a case controlled study. Eur J Obstet Gynecol Reprod Biol. 2014; 180: 93-99.
- De Leo V, Di Sabatino A, Musacchio MC, et Effect of oral contraceptives on markers of hyperandrogenism and SHBG in women with polycystic ovary syndrome. Contraception. 2010; 82: 276-280.
- Suvarna Y, Maity N, Kalra P, et al. Comparison of efficacy of metformin and oral contraceptive combination of ethinyl estradiol and drospirenone in polycystic ovary syndrome. J Turk Ger Gynecol Assoc. 2016; 17: 6-9.
- Guido M, Romualdi D, Giuliani M, et Drospirenone for the treatment of hirsute women with polycystic ovary syndrome: a clinical, endocrinological, metabolic pilot study. J Clin Endocrinol Metab. 2004; 89: 2817-2823.
- Pehlivanov B, Mitkov M. Efficacy of an oral contraceptive containing drospirenone in the treatment of women with polycystic ovary syndrome. Eur J Contracept Reprod Health Care. 2007; 12: 30-35.
- Nader S, Diamanti-Kandarakis Polycystic ovary syndrome, oral contraceptives and metabolic issues: new perspectives and a unifying hypothesis. Human Reproduction. 2007; 22: 317-322.
- Amiri M, Nahidi F, Khalili D, et Comparing the Effects of Oral Contraceptives Containing Levonorgestrel With Products Containing Antiandrogenic Progestins on Clinical, Hormonal, and Metabolic Parameters and Quality of Life in Women With Polycystic Ovary Syndrome: Crossover Randomized Controlled Trial Protocol. JMIR Res Protoc. 2017; 6: e191.
- Kriplani A, Periyasamy AJ, Agarwal N, et al. Effect of oral contraceptive containing ethinyl estradiol combined with drospirenone vs. desogestrel on clinical and biochemical parameters in patients with polycystic ovary syndrome. Contraception. 2010; 82: 139-146.
- Macut D, BožiÄ? AntiÄ? I, Nestorov J, et al. The influence of combined oral contraceptives containing drospirenone on hypothalamic-pituitary-adrenocortical axis activity and glucocorticoid receptor expression and function in women with polycystic ovary syndrome. Hormones (Athens). 2015; 14: 109-117.
- Ozdemir O, Sari ME, Kalkan D, et al. Comprasion of ovarian stromal blood flow measured by color Doppler ultrasonography in polycystic ovary syndrome patients and healthy women with ultrasonographic evidence of Gynecol Endocrinol. 2015; 31: 322-326.
- Amin AF, Abd el-Aal DE, Darwish AM, et al. Evaluation of the impact of laparoscopic ovarian drilling on Doppler indices of ovarian stromal blood flow, serum vascular endothelial growth factor, and insulin-like growth factor-1 in women with polycystic ovary syndrome. Fertility and Sterility. 2003; 79: 938-941.