Posterior Distal Para-Urethral Leiomyoma in Virgin Female Patient: A Case Report
Author’(s): Zwawa Alia1, Elmahaishi Wael2, Elmahaishi Hamza3, and Elmahaishi M.S.4
Gynecology Department, Lamis Clinic, Misurata / Libya.
*Correspondence:
Prof. Dr. Elmahaishi M.S., Lamis Clinic, P.O. Box. 65, Hospital road of Tripoli street, Misurata / Libya.
Received: 18 July 2020 Accepted: 14 August 2020
Citation: Alia Z, Wael E, Hamza E, et al. Posterior Distal Para-Urethral Leiomyoma in Virgin Female Patient: A Case Report. Gynecol Reprod Health. 2020; 4(5): 1-4.
Abstract
Paraurethral leiomyoma is a rare condition with less than 45 cases reported in the literature worldwide [1-14] Prompt diagnosis, especial needs to exclude malignant tumor. Proper treatment is necessary to prevent complications. Clinically is very difficult to distinguish from other urethral lesions, the diagnosis of leiomyoma is established by histopathological examination [7,15-16] Our case was different in that the mass was located in the posterior wall of distal urethra, which is not the common site of presentation of leiomyoma in females, our patient is a virgin women and also the leiomyoma was protruding outside the introits. She had no symptoms.
Keywords
Introduction
Leiomyomas are benign mesenchymal tumors that arise from the smooth muscle meanly located in genital tract. uterus is the most common site of Leiomyomas. Average age of patients presenting with Paraurethral leiomyoma is 39.8years [17]. Somewhat younger than average age of patients with afibroid uterus, they have also been found in older women, such as our patient [18]. Locations of leiomyoma in the genitourinary tract have been documented in the uterus, renal pelvis, ureter, bladder wall, and urethra in women [19]. However, leiomyomas arising from the female urethra, especially paraurethral, are exceedingly rare [20]. Of the reported urethral tumors, only a few have been reported as true paraurethral tumors [20-22]. A true paraurethral tumor is defined as a mesenchymal neoplasm growing in the paraurethral space without any communication with the urethra, bladder, or vagina [22-24]. We present a case of a paraurethral leiomyoma confirmed by Histopathological examination in a virgin woman. The size of tumor was more than 4cm in diameter.
Case Report
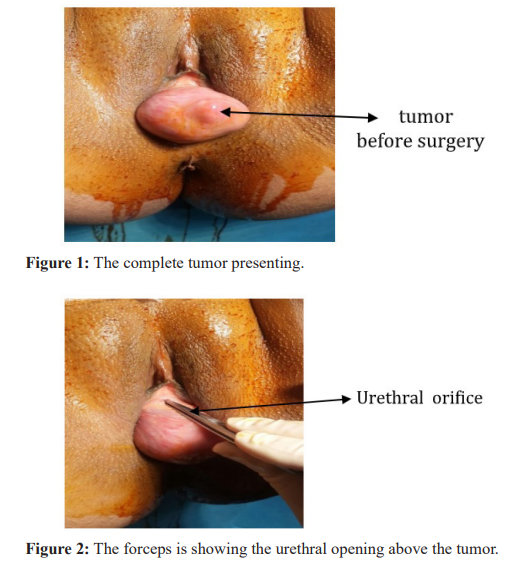
A 45-year-old female patient presented with swelling in the region of the posterior distal urethra, gradually increasing in size over the past 9 months. She had no history of hematuria, dysuria or voiding problems. Physical examination revealed a firm, mobile, non-tender mass sized 4.5 cm × 5 cm, located just posterior to the urethral meatus protruding outside the introits. The patient's results on routine investigations were within normal limits. Ultrasonography revealed a normal urinary system. Examination under anesthesia showed a mass arising from the posterior wall of the distal urethra protruding out from the introits. The remaining bladder and urethra were normal. The tumor was free from the urethra and not fixed to any structure and no sign of infiltration to the urethral wall or creatural vaginal walls.
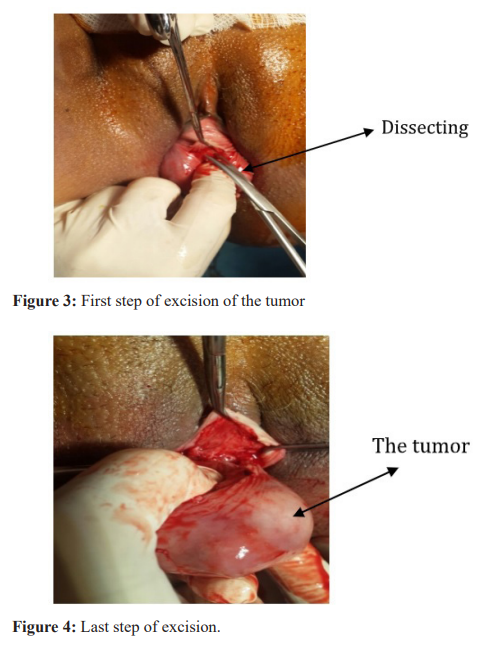
The mass was completely excised under general anesthesia. Histopathology revealed an encapsulated tumor containing spindle to plump oval nuclei-bearing cells with eosinophilic cytoplasm in collagenous tissue, suggesting a benign leiomyoma. On follow-up, the patient had no any clinical abnormalities or evidence of tumor recurrence.
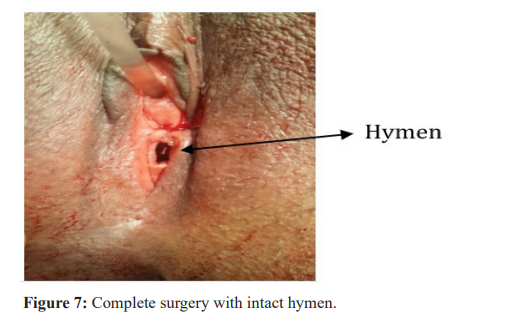
During the surgery the hymen kept intact urinary catheter inserted during the operation and kept for 24 hours.

Discussion
Leiomyoma of the urethra is a rare tumor, the first case described by BUTTNER in 1894 [20], the tumor is more common in women than in men, with an average age of onset of 40 years [20,25,26].
The exact etiology of this tumor is not known. Hormone cause is controversial [3,26]. Histologicaly the leiomyoma are tumors interesting the female genital tract, in the urethra it found mainly in the proximal portion (the posterior supace of the urethra ) is more affected [7,20].
Primary urethral leiomyoma is seen more frequently in females than in males, and it usually develops at the posterior wall of the proximal urethra [2], The most common symptom found in 50% of the cases is swelling near the periurethral region [4-6]. Other symptoms include hematuria, dysuria, repeated urinary tract infection and dyspareunia [3,7]. Obstructive voiding symptoms are rare due to the paraurethral rather than periurethral position of the neoplasm, while other patients may be completely asymptomatic [10]. As in our case. Only histopathological examination can distinguish leiomyoma from malignant tumor.
Simple surgical excision is the treatment of choice [9] and this is what was done in our case. Local recurrence after removal is possible but rare [7-20].
This case had no symptoms part from a mass protruding from vagina. It was increasing in size over last 9 months. Her thinking this mass could be a cancer. On clinical examination the differentials diagnosis includes urethral carcinoma, urethral caruncle, urethral diverticulum, vaginal wall cysts, endometriosis, duct abscess, fibroid, fibroepithelial polyp, adenomyoma [30-34].
Anatomic positioning. From anterior to posterior, there are four layers separating the exterior vaginal wall from the paraurethral space including epithelium, submucosa, fibromuscular banding containing smooth muscle, and periurethral fascia [28]. Urethral leiomyomas in women occur most commonly on the posterior urethral wall. However, vaginal wall leiomyomas most commonly occur on the anterior vaginal wall [29] occur between in the vesicovaginal septum paraurethral space in occupied our case the myoma. It is hypothesized that the extreme rarity of paraurethral leiomyoma is due to a drastic reduction of tissue found in the vesicovaginal septum or paraurethral space [30].
Differentiating the anatomical location of the leiomyoma by the clinical presentation is also not reliable. Signs and symptoms of vaginal, urethral, and paraurethral leiomyoma may present very similarly. Common complaints of all three include urinary tract infection, a mass, dyspareunia, urinary retention, hematuria, dysuria, dyspareunia, and obstructive voiding symptoms [27,31- 32]. Patients also may be completely asymptomatic. Overall. The age for these types of neoplasms ranges from 40 to 44 [33-34]. Like this case.
High-frequency transperneal ultrasound shows leiomyomas as solid tumors with a homogeneous internal echo structure. Ultrasound provides a quick and effective means of the mass localization in relationship to the urethra as wells as ruling out infiltration and diverticula. The result of our ultrasound showed the tumor is with identified boarder in para urethral space without any infiltration to adjacent tissue around.
A definitive diagnosis of parsurethral leiomyoma was made. Although the pathogenesis of vaginal, urethral, and paraurethral leiomyomas is not certain, Surgical intervention is the standard of care for symptomatic patients [30,33]. The surgical technique will differ according to the site of the mass. excision posterior paraurethral space out side the perennially resection in our patient was performed by opening the paraurethral space between the posterior distal urethral wall and anterior vag. wall.
According to Navarro et al. [35], paraurethral leiomyoma presented as benign neoplasms of mesenchymal origin contained in a fibrous capsule not adherent to adjacent structures [35], a histopathologic presentation identical to our case.
The place of the myoma was reconstructed to normal with out making any damage to the hymen. Urinary catheter was inserted for 24 hours then removed. Patient sent home without any complication. She was seen in the flow up gynecology clinic after 5 weeks without any remarks.
Conclusion
Posterior, distal paraurethral leomyon was excised from posterior paraurethral space without any complication. The hymen was intact and saved from any injury.
References
- Shield DE, Weiss RM. Leiomyoma of the female urethra. J Urol. 1973; 109: 430-431.
- Leidinger RJ, Das S. Leiomyoma of female urethra. A report of two cases. J Reprod Med. 1995; 40: 229.
- Lee MC, Lee SD, Kuo HT, et Obstructive leiomyoma of the female urethra: report of a case. J Urol. 1995; 153: 420-421.
- Cheng C, Mac-Moune Lai F, Chan PE. Leiomyoma of the female urethra: a case report and review. J Urol. 1992; 148: 1526-1527.
- Dmochowski R, Ganabathi K, Zimmern PE, et al. Benign female periurethral masses. J Urol. 1994; 152: 1943-1951.
- Castle W, McLaughlin MC. Paraurethral vaginal leiomyoma. Urology. 1987; 30: 70-72.
- Fry M, Wheeler Jr J, Mata J, et al. Leiomyoma of the female urethra. J Urol. 1988; 140: 613-614.
- Noto L. Obstructive urethral leiomyoma in a female. Br J Urol. 1983; 55: 239.
- Leung YL, Lee F, Tam PC. Leiomyoma of female urethra causing acute urinary retention and acute renal J Urol. 1997; 158: 1911-1912.
- Di Cello V, Saltutti C, Mincione G, et al. Paraurethral leiomyoma in women. EurUrol. 1988; 15: 290-293.
- Sangwan K, HuriaKhosla A, Hazra P. Leiomyoma of the vagina. Aust NZ J ObstetGynaecol. 1996; 158: 494-495.
- Joshi HB, Beck Leiomyoma of the female urethra with upper tract dilatation and treatment with transurethral resection: a case report and literature review. Tech Urol. 2000; 6: 223-225.
- Goldman HB, McAchran SE, MacLennan Leiomyoma of the urethra and bladder. J Urol. 2007; 177: 1890.
- Merrell RW, Brown HE. Recurrent urethral leiomyoma presenting as stress incontinence 1981; 17: 588-589.
- Deka P, Rajeev T. Leiomyoma of the female urethra. A case report. Urol Int. 2003; 71: 224-225.
- Diószeghy G, Kiss A, Kondas J. Leiomyoma of the female urethra. IntUrolNephrol. 1998; 30: 603-637.
- Goluboff ET, Toole KO, Sawczuk Leiomyoma of bladder: report of case and review of literature. Urology. 1994; 43: 238-241.
- Shim S, Borg CS, Majeed HG, et Paraurethral Leiomyoma in a Postmenopausal Woman: First European Case. Case Reports in Obstetrics and Gynecology. 2015; 1-3.
- Belis JA, Post GJ, Rochman SC, et al. Genitourinary leiomyomas. Urology. 1979; 13: 424-429.
- Blaivas JG, Flisser AJ, Bleustein CB, et al. Periurethral masses: etiology and diagnosis in a large series of women. ObstetGynecol. 2004; 103: 842-847.
- Tunitsky E, Goldman HB, Ridgeway Periurethral mass: a rare and puzzling entity. ObstetGynecol. 2012; 120: 1459-1464.
- Di Cello V, Saltutti C, Mincione GP, et al. Paraurethral leiomyoma in women. EurUrol. 1988; 15: 290-293.
- Selli C, Dal Canto M, Campani D, et al. Leiomyoma of the female urethra. UrolInt. 1995; 54: 179-180.
- Cheng C, Mac-Moune Lai F, Chan PS. Leiomyoma of the female urethra: a case report and review. JUrol. 1992; 148: 1526-1527.
- Chang S, Cooperberg P, Wong A, et al. Limited-sequence magnetic resonance imaging in the evaluation of the ultrasonographically indeterminate pelvic mass. Can AssocRadiol J. 2004; 55: 87-95.
- Lake M, Kossow A, Bokinsky G. Leiomyoma of the bladder and urethra. J Urol. 1981; 125: 742-743
- Chang C, Mac-Moune Lai F, Chan PS. Leiomyoma of the female urethra: a case report and review. J Urol. 1992; 148: 1526-1527.
- Dmochowski RR, Ganabathi K, Zimmern PE, et al. Benign female periurethral masses. J Urol. 1994; 152: 1943-1951.
- Castle WN, McLaughlin Paraurethral vaginal leiomyoma. Urology. 1987; 30: 70-72.
- Martin JH, Gerrard Parauethral Leiomymoa: Does Making the distinction Make a difference ?. infect Urol. 2001; 14.
- Bruschini H, Truzzi JC, Simonetti R, et al. Paraurethral leiomyoma in a female causing urinary obstruction. Int Urogynecol J Pelvic Floor Dysfunct. 2006; 17: 286-289.
- Giacomo Perugia, Mauro Ciccariello, Francesca Pirolli, et al. Paraurethral leiomyoma. Urology. 2012; 79: e51-e 52.
- Cornella JL, Larson TR, Lee RA, et al. Leiomyoma of the female urethra and bladder: reports of twenty -threepatients and review of the Am J Obstet Gynecol. 1997; 176: 1278-1285.
- Cattolica EV, Klein R, Knigge Paraurethral leiomyoma- an imitator. Urology. 1976; 8: 605-607.
- Pastor Navarro H, Martinez Ruiz J, Martinez Sanchiz C, et Paraurethral Leiomyoma. Arch Esp Urol. 2013; 66: 820-823.