Postmyomectomy Hemoperitoneum: A Rare Cause of Acute Intestinal Obstruction: A Case Report
Author'(s): Adjoby Roland1, Gbary-Lagaud Eleonore1, Koffi Soh Victor1, Effoh Ndrin Denis1, Akobe Privat1, Kouakou-Kouraogo Ramata1, Nguessan-Yapi Francis1, and Soro Ngolo Alassane2
1Gynecology and Obstetrics Department at the Teaching Hospital of Angré, Côte d’Ivoire.
2Anesthesia, Resuscitation Department at the Teaching Hospital of Angré, Côte d’Ivoire.
*Correspondence:
Adjoby Roland, Gynecologist, Gynecology and Obstetrics Department at the Teaching Hospital of Angré, Côte d’Ivoire.
Received: 08 June 2020 Accepted: 01 July 2020
Citation: Adjoby Roland, Gbary-Lagaud Eleonore, Koffi Soh Victor, et al. Postmyomectomy Hemoperitoneum: A Rare Cause of Acute Intestinal Obstruction: A Case Report. Gynecol Reprod Health. 2020; 4(4): 1-4.
Abstract
We report the case of a G4P2 of 41 years of age presenting a bulky fibromatous uterus of size 22-24 weeks, having undergone a polymyomectomy under cervical-isthmic tourniquet for desire of maternity after an injection of LHRH agonist. The post-operative complications were complicated by acute intestinal obstruction. An exploratory laparotomy has objectified a residual hemoperitoneum of low abundance and a solid adhesion between the posterior surface of the uterus and the ileum at the level of post myomectomy hysterorraphy. The conservative treatment consisted of a lifting of the occlusion by careful adhesiolysis, without intestinal resection. This case illustrates the morbidity of post myomectomy bleeding linked to the adhesiogenic activity of fibrin.
Keywords
Introduction
Myomectomy is one of the most common surgical procedures in Africa in the face of multiple complications of uterine fibroids, including infertility [1]. This conservative intervention of the uterus in women often in full genital activity gives them a chance of conception. Myomectomy, however, has a certain morbidity and even mortality, including acute intestinal obstruction [2]. We report a rare case of occlusive syndrome by early adhesion of intestinal loop on the posterior surface of the uterus.
Observation
TML 41-year-old patient G4P1 (2 abortions, 1 4-year-old daughter), accountant, with no particular medical-surgical history, followed for secondary infertility for 2 years, diagnosed with a polyfibrous uterus of size 22-24 weeks of amenorrhea including 2 posterior development fundus intramural nuclei with a mass effect on the endometrium.
In view of the desire for motherhood, it was decided and realized in her a polymyomectomy without mucous membrane break, under isthmic cervical tourniquet after an injection of LHRH agonist.
The immediate consequences were marked by a slight anemia at 9g / dl and an occlusive syndrome on D7 marked by an incomplete cessation of materials and gases and early vomiting after attempting to eat food. A digestive surgeon's opinion confirmed the clinical impression, with a slightly meteorized abdomen and very sensitive as a whole, and a presence of stool on the digital rectal examination, the x-ray of the abdomen without preparation was in favor of centered and stepped hydroaeric levels (Figure 1).
After unsuccessful medical management attempts with nasogastric probe and evacuating enema through Normacol®, and hydroelectrolyte rehydration, an exploratory laparotomy was indicated for high suspicion of occlusion. An exploratory laparotomy will objective a residual hemoperitoneum of low abundance (400cc) and a strong adhesion between the posterior surface of the uterus and the ileum at the level of the post myomectomy hysterorraphy (Figures 2 and 3). This adhesion was 50 cm from the ileo-caecal junction, next to a hystererorraphic suture, without a necrosis zone.

Figure 1: X-ray of the abdomen without preparation.

Figure 2: Intestinal loop after adhesiolysis.

Figure 3: Intestinal loops bent upstream of the adjoining area.
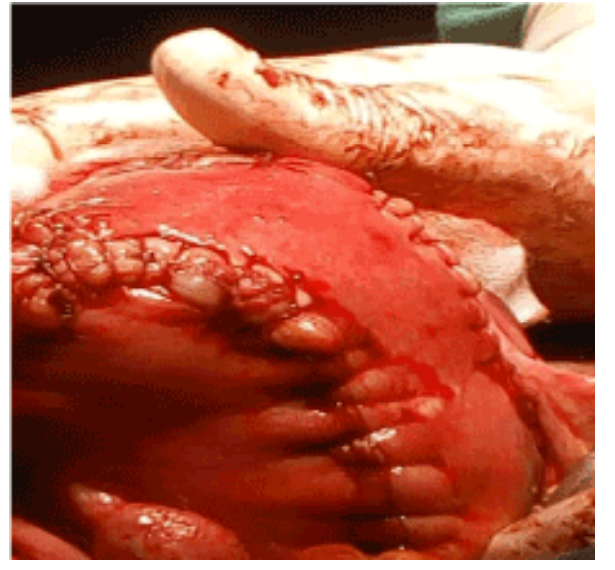
Figure 4: Posterior surface of the uterus after myomectomy.
The conservative treatment consisted of the removal of occlusion by conservative adhesiolysis. Clots were also noted in the hysterorrhaphy sutures and the stool was repelled to check the permeability of the adherent area not requiring intestinal resection. Extensive washing of the abdominal cavity was performed with physiological serum prior to closing the abdomen. Surgical follow- ups were simple with resumption of transit.
Discussion
Epidemiology
The incidence of adhesions after digestive surgery is 94%, and after gynecological surgery is 60-90%. Open-stomach polymyomectomy is one of the most adhesive gynecological procedures after endometriosis surgery and tubal surgery [2-4].
Myomectomy is one of the most common procedures in gynecological surgery in Black Africa, given the frequency that varies from 25 to 40% in black women [4]. The early onset of occlusive syndrome due to post-myomectomy adhesions is a rare complication [1,5].
Etiopathogenesis
Adhesions are fibrous tissues that viciously and physically unite the surfaces of tissues that are naturally contiguous, but separate. The union of tissue surfaces via adhesions can take two forms: either in the form of direct joining (welding) of the surfaces of contiguous tissues via fibrous tissue freshly or formerly formed; either indirectly through fresh or formerly formed fibrous tissues and in the form of veils, bands, bridles, ropes and pillars of varying thickness, varying length and sometimes vascularized [1,5,6].
At the level of the injured surfaces a cascade of events occurs leading to the formation of adhesions: inflammatory reaction, increase in microvascular permeability, formation of inflammatory exudation with deposits of fibrin and invasion by fibroblasts resulting in the formation of fibrous tissue connecting the traumatized tissues. The adhesion formation mechanism begins during the intervention and is completed 3 to 5 days after the intervention is completed [1].
The management of adhesions consists of careful adhesiolysis to avoid any deceritonization [1,7]. In our case, it was a solid ileo- uterine adhesion, favored by the residual hemoperitoneum post myomectomy, having led to acute intestinal obstruction. Indeed, a fibrin matrix is created on the site of the trauma and forms a bridge on the adjacent surfaces (ileum and hysterorraphy area). Small bowels are linked to the presence of intra-abdominal adhesions in 74% of cases; they occur in principle long after the surgical procedure [1,2]. In our observation, this occlusion occurred early in a week. In the literature, it was established that utero-adnexal adhesions are significantly more frequent with posterior incisions compared to fundic or anterior incisions [1].
The practice of hemoperitoneum drainage is not systematic in our practice. We perform myomectomy under cervical isthmic tourniquet associated with the placement of abdominal drapes to reduce intra-abdominal bleeding [8,9]. After adhesiolysis, the risk of recurrence of adhesions to the site of this surgical procedure is around 85% [2].
How to prevent adhesions?
Several recommendations have been set out, including handling the tissues with care using surgical magnification techniques for more precise and gentle surgery. Avoid handling structures that are distant from the operating site and reduce bleeding, as blood increases the risk of adhesion formation. Carry out a careful hemostasis while ensuring that cauterization is used with caution. Cauterization causes peritoneal trauma and stimulates the formation of adhesions. Reduce tissue drying (limit heat and lighting) and avoid packing the intestine. Prefer overlocking at separate points on the uterus and avoid the use of dry towels or sponges in laparotomic surgery [1,2,5].
In order to reduce the risk of formation of post-operative adhesions, some centres use anti-adhesion agents: either in the form of films which can constitute a translucent and temporary mechanical barrier at the level of the operative site in order to separate the surfaces of contiguous tissues.
They should not be placed around the anastomoses due to the risk of fistula. Some anti-adhesion films are composed of two chemically modified anionic polysaccharides: sodium hyaluronate and carboxymethylcellulose (CMC); the films are transformed into gel after 24 hours after installation and they are normally absorbed at the operating site in one week and their components are completely excreted from the body in 28 days, via the kidneys [2]. Or in the form of a viscous gel composed of pure cross- linked hyaluronate (hyaluronic acid) which can be applied to the operating site: ovarian surgery, fallopian tubes, uterine sutures, treated endometriotic lesions, adhesiolysis site, surgery the uterine cavity. Or in the form of a solution (icodextrin at 4%) which makes it possible to create a hydroflottation, with the maintenance of ascites for 3 to 4 days separating the surfaces of the tissues from the operating site. Polyethylene glycol gel is also used as anti-adhesion; it is absorbable in 5 to 7 days [2,10]. However, the effectiveness of these techniques remains much debated, Tulandi and al found an incidence of slightly higher complications when using barrier methods [11].
Conclusion
Uterine myoma surgery is highly adhesiogenic. This adherent potential could be the cause of occlusive syndromes in the immediate post-operative, hence the interest of working to its prevention by the strict application of the anti-adherent mechanisms. This case illustrates the morbidity of post-myomectomy bleeding or hemoperitoneum, related to the adhesiogenic activity of fibrin.
References
- Le Tohic A, Niro J, Panel Myomectomies: techniques pour optimiser la fertilité, 36è journées CNGOF, Paris. 2012; 241- 259.
- Pouly JL, Darai EC, Yazbzck JL, et al. Adhérences postopératoires et leur prévention en chirurgie gynécologique: comment les prévenir ? Journal Obstétrique, Gynécologie & Fertilité. 2012; 40: 7-9.
- Foulot H, Chopin N, Malartic C, et al. Myomectomies par laparotomie. EMC, Techniques chirurgicales-Gynécologie. 2005; 2: 41-662.
- Koffi ABD, Olou NL, Fomba M, et Chirurgie des fibromes utérins: bilan de cinq années d’activités au service de gynécologie du CHU de Yopougon. Rev Int Sc Méd. 2013; 2: 95-99.
- Lee ET, Wong FW. Small bowel obstruction from barbed suture following laparoscopic myomectomy-A case Int J Surg Case Rep. 2015; 16: 146-149.
- Gavai M, Berkes E, Fekete E, et al. Analysis of perioperative morbidity according to wether the uterine cavity is opened or remains closed during abdominal myomectomy- result of 423 abdominal myomectomy Clinical Exp Obstet Gynecol. 2008, 35: 107-112.
- Schwenter F, Dominguez S, Meier R, et al. Occlusion grêle aiguë: traitement conservateur ou chirurgical? Rev Med Suisse. 2011; 7: 1341-1347.
- Fanny M, Fomba M, Aka E, et al. Prevention of bleeding during laparotomic myomectomy in Sub-Saharan Africa: Contribution to the tourniquet on the uterine Gynecol Obstet Fertil Senol. 2018; 46: 681-685.
- Ymele FF, Tsuala JF, Fouedjio JH, et al. Une complication rare des léiomyomes utérins: hémopéritoine massif par rupturede varices. Pan African Journal. 2013; 14: 110-115.
- Brown CB, Anthony A Luciano, Dan C Martin, et al. Adept (icodextrin 4% solution) reduces adhesion after laparoscopic surgery for adhesiolys a double-blind, randomized, controlled study. Fertil Steril. 2007; 88: 1413-1426.
- Tulandi T, Closon F, Czuzoj-Shulman N, et al. Adhesion Barrier Use After Myomectomy and Hysterectomy: Rates and Immediate Postoperative Obstet Gynecol. 2016; 127: 23-28.