Prevalence, Perception and Pattern of Peripheral Neuropathy among Pregnant Women in South-Eastern Nigeria
Author'(s): Adinma JIB1*, Adinma ED2, Umeononihu OS1, Oguaka V1, and Oyedum SO3
1Department of OBS/GYN, Nnamdi Azikiwe University and Teaching Hospital, Nnewi, Anambra State, Nigeria.
2Department of Community Medicine, Nnamdi Azikiwe University and Teaching Hospital, Nnewi, Anambra State, Nigeria.
3Department of Physiotherapy, Nnamdi Azikiwe University and Teaching Hospital, Nnewi, Anambra State, Nigeria.
*Correspondence:
Adinma J.I.B, Department of OBS/GYN, Nnamdi Azikiwe University and Teaching Hospital, Nnewi, Nigeria, Tel: +2348037080814; E-mail: brianadinma@yahoo.com.
Received: 09 May 2017 Accepted: 15 June 2017
Citation: Adinma JIB, Adinma ED, Umeononihu OS, et al. Prevalence, Perception and Pattern of Peripheral Neuropathy among Pregnant Women in South-Eastern Nigeria. Gynecol Reprod Health. 2017; 1(1): 1-5.
Abstract
Objectives: Neuropathies can complicate pregnancy, labour and delivery. To determine the prevalence and pattern of neuropathies among pregnant women.
Methods: Cross-sectional questionnaire-based study of 115 pregnant women attending antenatal-care outreaches in South Eastern Nigeria.
Results: Majority (45.2%) of the respondents were, aged 26-30 years; of parity 1 to 4, 79 (68.7%); and of social class 3, 64 (55.7%). Up to 60 (52.2%) of the respondents had heard of neuropathies in pregnancy. About 24.3% thought neuropathies occur from increase blood pressure; 28.7%, from pressure of bones on the nerves; while 33% agreed neuropathies could be treated with exercise. Twenty-eight (24.3%) respondents had experienced neuropathy in the index pregnancy. Neuropathies occurred more frequently at term gestational age, extremes of parity, and decreasing social class. Femoral nerve palsy was the most commonly experienced neuropathy (32.1%). Up to (42.9%) of respondents with neuropathy receive no treatment.
Conclusion: This study indicates appreciable knowledge of neuropath in pregnancy, low prevalence and distorted perception. A high index of awareness of neuropathy, knowledge of the treatment modalities and in-cooperation in to pregnancy health talk will improve perception and treatment, and reduce the burden of Neuropathies on pregnant women.
Keywords
Introduction
Peripheral nerves are susceptible to a variety of toxic, inflammatory, infectious, and parainfectious factors that can impair their health and function, leading to the clinical disorder of polyneuropathy. Peripheral neuropathy is a term that is frequently used synonymously with polyneuropathy, but can also refer to any disorder of the peripheral nervous system including radiculopathies and mononeuropathies [1].
A number of neuropathies can occur in pregnancy and postpartum. These include; carpal tunnel syndrome (CTS), Bell’s palsy, meralgia paraesthetica, Guillain-Barre syndrome, intercostal neuralgia, brachial plexus neuralgia and post-partum compression neuropathies. Carpal tunnel syndrome (CTS) refers to pain, or numbness along the distribution of the median nerve viz; the thumb, index, and middle fingers, due to compression of the median nerve in the carpal tunnel. The incidence in pregnancy is 2 to 35% [2]. Meralgia paraesthetica is a sensory neuropathy that occurs as a result of compression of the lateral femoral cutaneous nerve as it pierces the tensor fascia lata at the inguinal ligament. It manifests as dysesthesias in the upper and middle part of the lateral thigh and is thought to be due to the expanding abdominal wall and increased lumbar lordosis. It rarely requires treatment [3].
Bell's palsy (BP) is the paralysis of the facial nerve, typically involving all three peripheral branches, resulting in asymmetric facial expression and unilateral weakness of eye closure. Its prevalence doubles during pregnancy [4], believed to be due to relative immunosuppression in pregnancy, perineural oedema and hypercoagulability causing thrombosis of the vasa nervosum [5]. Guillain-Barré syndrome is an acute inflammatory demyelinating polyradiculoneuropathy (AIDP) linked to a variety of infectious agents. Its frequency is not increased during pregnancy nor does it have affect pregnancy and its outcome when uncomplicated [6].
Intercostal neuralgia results from increased intercostal nerve irritation due to rib subluxation that may occur in pregnancy. Brachial plexopathy also called brachial plexus neuropathy or Pancoast syndrome is pain, decreased movement, or decreased sensation in the arm and shoulder resulting from involvement of the brachial plexus as they leave the neck and enter the arm. Other neuropathies that can occur intrapartum or during the postpartum period include postpartum compression neuropathies [7] involving femoral and lateral femoral cutaneous nerves; peroneal nerve compression with foot drop; compression of the lumbosacral trunk which can also result in foot drop [8]; and obturator neuropathy which can present with media thigh pain and adductor weakness, with good prognosis, recovery occurring within 6-8 weeks [9].
This study has been undertaken among pregnant women attending antenatal clinical outreach in South Eastern Nigeria to determine their knowledge of, perceptions on, as well as the prevalence and pattern of neuropathies occurring during pregnancy. Findings from this study are expected to bridge information gap on this nagging condition that may occur during pregnancy and thereby improve its awareness, and knowledge of the treatment modalities among health providers caring for pregnant women.
Materials and Methods
This is a questionnaire-based, interviewer-administered cross- sectional study of 115 antenatal clinic attendees during two free antenatal care outreach programmes conducted at two locations – Nnewi and Nkpor in Anambra State of South Eastern Nigeria, in 2015. Only pregnant women attendees who gave their consent were drawn into the study. Oral consent was obtained from the participants after due explanation of the objective of the study. The questionnaires were administered by trained interviewers, consisting of clinical medical students and students of physiotherapy, under the supervision of consultant obstetrician and gynaecologist. The questionnaire-schedule elicited information from the respondents with respect to their biosocial characteristics - age, parity, gestational age, and social class; their knowledge of and perception on neuropathies with respect to causes, consequences and treatment; presence of neuropathy in the current or immediate past pregnancy. The social class of the respondents was derived from Olusanya classification which makes use of educational level of the woman and the occupation of her husband [10]. The Neuropathy Index (NI) was calculated by dividing the Number of Neuropathy cases (Nc) by the Number of Respondents (Nr). The Neuropathy Index (NI) was calculated for the stems of the variables. Data from the completed questionnaire were keyed into the system and analysed using SPSS version 17.0. Statistical relationships between variables were calculated using the Chi- square test and a p-value of <0.05 at 95% confidence interval was considered significant for all statistical comparison. Analysed data were displayed in tables.
Results
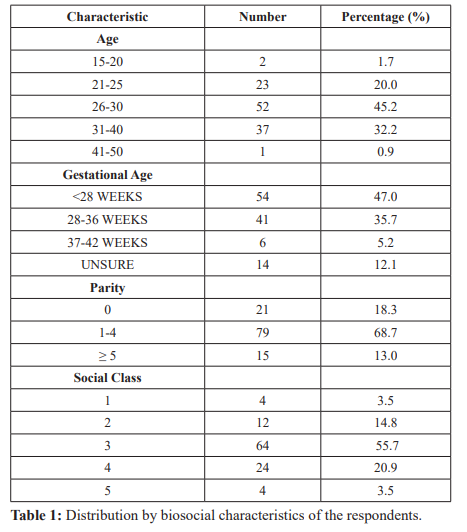
One hundred and fifteen participants were involved in the study. Table 1 shows the distribution by the biosocial characteristics of the respondents. Majority of the respondents were within the age range 26-30 years, 52 (45.2%); were multiparous i.e Para 1-4, 79 (68.7%); and were of Social class 3, 64 (57.5%). Majority of the respondents were less than 28 weeks gestational age, 54 (47.0%) followed by those between 28 and 36 weeks, 41 (35.7%).
The distribution by knowledge and perception of neuropathies for the respondents as shown in Table 2 indicates that up to 60 (52.2%) respondents have heard of neuropathies associated with pregnancy, while 55 (47.8%) had not. Almost an equal number of the respondents 28 (24.3%) and 29 (25.2%) respectively perceived, and did not perceive that neuropathies are caused by rise in blood pressure, while as high as 57 (49.6%) did not know. Up to 33 (28.7%) respondents believed that neuropathies are related to pressure of bones on the nerves, while 25 (21.7%) did not. As high as 57 (49.6%) had no knowledge of this. Similarly up to 33 (28.7%) respondents believed that neuropathy are associated with paralysis while 23 (20%) did not. As high as 59 (51.3%) had no knowledge. Whereas 26 (22.6%) respondents believed that neuropathies can cause miscarriage or premature birth, 22 (14.1%) did not, while majority of the respondents 67 (58.3%) did not know. An almost equal number of respondents 29 (25.2%) and 31 (26.9%) respectively believed that neuropathy can affect labour/ delivery, and cannot, while as high as 55 (47.8%) did not know. Up to 39 (33.9%) of respondents believed that neuropathies can be treated by exercise while 21 (18.3%) believed it cannot. As high as 55 (47.8%) respondents did not know.
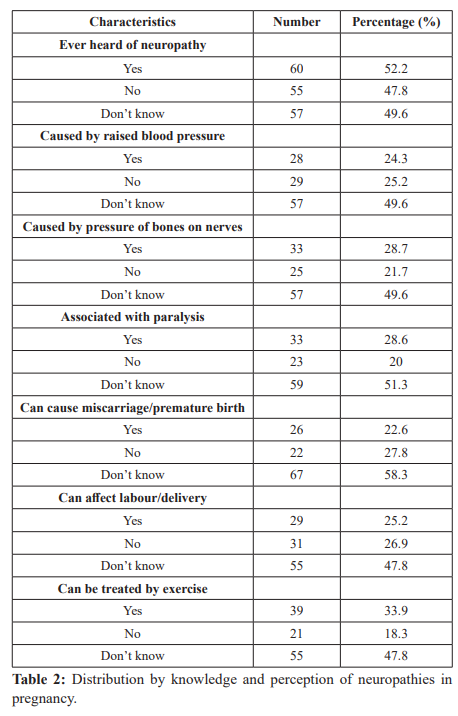
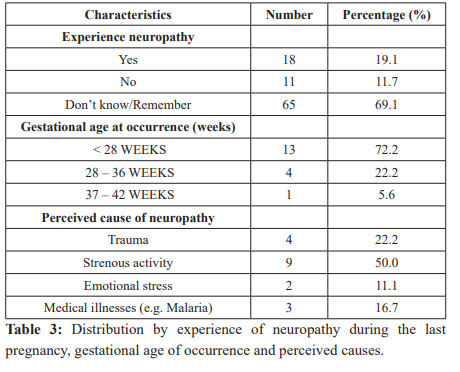
Table 3 shows the distribution by experience of neuropathies in the last pregnancy, gestational age at occurrence and perceived cause of the neuropathy by respondents. Eighteen (19.1%) of the 94 respondents involved experienced neuropathy, 11 (11.7%) did not, while 65 (69.1%) could not remember. Majority 13 (72.2%) of the respondents experienced neuropathy at gestational age less than 28 weeks, 4 (22.2%) had experienced it between 28 to 36 weeks, while only 1 (5.2%) had experienced neuropathy at gestational ages of 36 weeks and above. Trauma was believed to be the cause of neuropathy in pregnancy 4 (22.2%), strenuous activity 9 (50%), emotional stress 2 (11.1%) and medical illnesses 3 (16.7%).
The distribution by experience of neuropathy in the current pregnancy, types of neuropathy experienced, gestational age at occurrence and treatment receive is shown in Table 4. Neuropathy was experienced in 28 (24.3%), 61 (53.0%) did not, while 26 (22.6%) had no knowledge of whether they did or not. The most common form of neuropathy experienced was femoral nerve palsy 9 (32.1%) followed by carpal tunnel syndrome 6 (21.4%) while the least was Bell’s palsy 2 (7.1%). Majority of the neuropathies occurred among respondents of gestational age less than 28 weeks 18 (64.3%), while 7 (25.0%) occurred at 28 to 36 weeks and 3 (10.7%) occurred 37 weeks and above. Among treatment given for neuropathies include none, 12 (42.9%); Oral analgesics 6 (21.4%); Exercise 5 (17.9%); Rest 4 (14.3%) and Embrocation (Balm) 1 (3.6%).
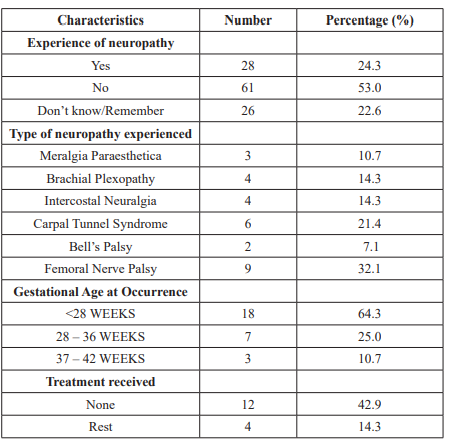
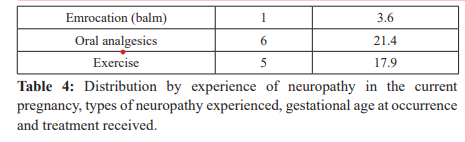
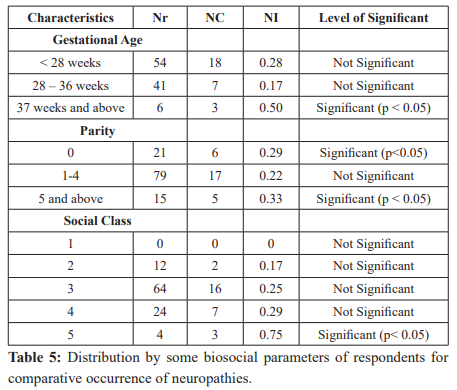
Table 5 shows the distribution by some biosocial parameters of respondents for comparative occurrence of neuropathies (Neuropathy Index (NI). Neuropathies occurred more significantly at gestational ages of 37 weeks and above, (NI = 0.50) compared to that of gestation ages of less than 28 weeks (NI = 0.28) and that of 28 to 36 weeks (NI = 0.17) (P<0.05). It also significantly occurred at extremes of parity – Para 0 (NI = 0.29) and Para 5 and above (NI = 0.33) compared to the middle parity group Para 1-4 (NI = 0.22) (P<0.05). Neuropathies occurred with increasing social class. There was none among respondents of Social class 1. Neuropathy Index was 0.17 for respondents of social class 2; Social Class 3, (NI = 0.25); Social Class 4 (NI = 0.29) and increasing to significant level of (NI = 0.75) for respondents of Social Class 5 (P<0.05).
Discussion
Information on Neuropathy in pregnancy in Nigeria is virtually absent in the literature. This perhaps may be due to the general believed that peripheral neuropathy is uncommon in pregnancy [11]. In this study the incidence of peripheral neuropathy in the index pregnancy, of 24.3%, seems low, but may in fact constitute a gross under-representation of the true incidence of the disease among Nigerian pregnant women. Considered from the observation in study that as high as 47.8% of the respondents had not heard of neuropathy in pregnancy, and further more a considerable number of the respondents, ranging between 47.8% and 58.3% had no knowledge of any perceptions on neuropathies in pregnancy. The current study shows how common some of these neuropathies may be. The level of knowledge of the respondents about neuropathy seems appreciable, as up to 52.2% of respondents are aware of the disorder. However the respondents’ knowledge of the causes and consequences of neuropathy in pregnancy is low, and this is compounded by the significantly high number of them with wrong perceptions on neuropathy in pregnancy.
In this study, neuropathies occurred most frequently at term gestational age. This is probably because of the increased likelihood of pressure and other symptoms of pregnancy such as oedema. Neuropathy was also more common at extremes of parity. The reason for this is not clear, it is however tempting to suggest a relationship between the occurrence of neuropathy and high risk obstetrics situations of which the extreme parity groups constitute. The incidence of neuropathy was also observed to increase with decreasing social class with a neuropathy index of zero among respondent of social class one, rising to significant level of 0.75 among the pregnant women of social class five. This therefore implies that pregnant women of lower social class tend to experience neuropathy more often than those of higher social class.
The femoral nerve palsy has a prevalence of 7.8% among the respondents and accounts for 32.1% of cases of neuropathies thereby making it the commonest type of neuropathy among the population under study. This is in contradistinction to the finding in a previous study where it constitutes only 1% of all mononeuropathies. This disparity may be due to the fact that pregnancy confers additional risk to the development of femoral neuropathy.
The prevalence of carpal tunnel syndrome (CTS) is also high among the respondents and accounts for 24.1% of those with neuropathies. This is comparable to the finding in a previous study [2]. CTS is relatively common during pregnancy, with an incidence of 2 to 35% [2]. In a large series, pregnancy accounted for 7% of cases of CTS in women between the ages of 15 and 44 [12]. The increased prevalence in pregnant women is thought to be caused by pregnancy-related fluid-retention leading to compression of the nerve in the carpal tunnel, and also hormonal changes affecting the musculoskeletal system.
Bell’s palsy was documented in 2 of the respondents accounting for 7.1% of all those with neuropathies. In the United States of America, the annual incidence of Bell’s palsy is approximately 23 cases per 100,000 persons in the general population [13].
Studies have shown that pregnant women have a 3.3 times higher risk of being affected by Bell’s palsy than non-pregnant women and that it occurred more frequently in the third trimester [14]. The two cases of Bell’s palsy in this study occurred in the third trimester. Meralgia paraesthetica was seen in 2.6% of the respondents in this study, and accounted for 10.7% of neuropathies recorded. Pregnancy increases the risk of meralgia paraesthetica probably because of the compression of the lateral femoral cutaneous nerve as it penetrates the tensor fascia lata at the inguinal ligament by the expanding abdominal wall, and increased lumbar lordosis.
Symptoms occur late in pregnancy, typically resolve within three months postpartum, and rarely require treatment. In the general population, an incidence of 4.3 per 10,000 person years has been reported [15].
Brachial plexopathy though a rare disorder accounting for 14.3% of those with neuropathies. Idiopathic brachial plexopathy has an estimated annual incidence of 2 to 3 per 100, 000 [16,17]. In one large series, the male to female ratio was 2:1 [18]. Suggesting that the disorder may be commoner than initially thought especially among pregnant women.
Intercostal neuralgia is equally rare in the general population but was relatively common in this study accounting for a prevalence of 3.5% in the population under study. Treatment should be given for neuropathy during pregnancy when complaints occur, because of its notoriety for being burdensome. It is recommended that treatment should best approach the underlying cause of the neuropathy. Several forms of treatment have been recommended which includes the use of chiropractic care, massage, meditation, acupuncture, yoga, or even cognitive therapies. Others include safe nutritional supplements such as vitamin E, vitamin B12 and other prenatal drugs [11,19].
In this study, 42.9% of the respondents received no treatment for their neuropathic syndrome. Treatment given included oral analgesics 21.4%; exercise 17.9%; rest 14.3% and embrocation (balm) 3.6%. This pattern of treatment and in particular the high percentage of the respondents not given treatment at all is perhaps a pointer to the low awareness of the healthcare providers as to the prevalence of neuropathies in pregnancy together with the modalities of treatments available.
Conclusion
In conclusion the prevalence of neuropathy in pregnancy in Nigeria maybe much more than presently envisaged. A variety of neuropathies are commoner in pregnancy than in the general population. Hormonal changes and fluid retention with resultant weight changes in pregnancy may be responsible for these peculiarities. This study shows that neuropathy is commoner at term gestational age, at extremes of parity, and with decreasing social class. Knowledge of neuropathy among respondents in this study is reasonable but their perception to the causes and complications are distorted. The high percentage of the respondents with neuropathy in pregnancy did not receive any treatment for the condition, indicating the likelihood of a low awareness of neuropathies together with their treatment modalities by the healthcare providers. Healthcare practitioners should be properly enlightened on the possibility of neuropathy occurring in pregnant women as well as the treatment options available for them. Antenatal Health education program should incorporate the symptoms, complications and treatments of neuropathy during pregnancy to increase the awareness among the antenatal pregnant women. This will go a long way towards reducing the burden of neuropathy during pregnancy.
Acknowledgment
We are grateful to South East PAC-Net (SE-PAC-Net) for supporting this work carried out during its free antenatal care outreach programmes.
References
- Seward B, Rutkove SB, Shefner JM, et al. Overview of Polyneuropathy. Uptodate, Topic 5284 Version 10.0. 2012.
- Mabie WC. Peripheral neuropathies during pregnancy. Clin Obstet Gynecol. 2005; 48: 57.
- Men-Jean Lee M-J, Hickenbottom S, Aminoff MJ, et al. Neurologic Disorders Complicating Pregnancy. Uptodate Topic 4838 Version 11.0. 2013.
- Vrabec JT, Isaacson B, Van Hook Bell's palsy and pregnancy. Otolaryngol Head Neck Surg. 2007; 137: 858.
- Sax TW, Rosenbaum RB. Neuromuscular disorders in pregnancy. Muscle Nerve. 2006; 34: 559.
- Chan LY, Tsui MH, Leung TN. Guillain-Barré syndrome in pregnancy. Acta Obstet Gynecol Scand. 2004; 83: 319.
- Wong CA, Scavone BM, Dugan S, et Incidence of postpartum lumbosacral spine and lower extremity nerve injuries. Obstet Gynecol. 2003; 101:279.
- Marsh M. The Nervous System in Pregnancy. Glob Libr Women's Med. 2008.
- http://emedicine.medscape.com/article/1141793-overview
- Olusanya O. An original system of social classification for use in Nigeria and other developing countries. Presented at the 24th Annual Conference on the West African College of Surgeons Freetown, Sierra Leone January 1984.
- Massey E. Peripheral neuropathy in pregnancy. Phys Med Rehabil Clin N Am. 2008; 19: 149-162.
- Stevens JC, Beard CM, O'Fallon WM, et al. Conditions associated with carpal tunnel syndrome. Mayo Clin Proc. 1992; 67: 541.
- http://emedicine.medscape.com/article/1146903-overview7
- Katusic SK, Beard CM, Wiederholt WC, et Incidence, clinical features, and prognosis in Bell's palsy, Rochester, Minnesota, 1968-1982. Ann Neurol. 1986; 20: 622-627.
- Beghi E, Kurland LT, Mulder DW, et al. Brachial plexus neuropathy in the population of Rochester, Minnesota, 1970- 1981. Ann Neurol. 1985; 18: 320.
- http://emedicine.medscape.com/article/1141848-overview#a6
- MacDonald BK, Cockerell OC, Sander JW, et al. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain. 2000; 123: 665.
- Van Alfen N, van Engelen BG. The clinical spectrum of neuralgic amyotrophy in 246 cases. Brain 2006; 129: 438.
- Neuropathy Treatment Group. Dealing with pregnancy while having neuropathy; Nerve Renew. Neuropathy treatment group.