Study on the Relationship between Coping Style, Social Support and Quality of Life in Breast Cancer Surgery
Author'(s): Qiong DAI1 M.D, Jianqiong Liu1 M.D, Bei LIU3 M.D, Yanqin WANG1* M.B., Yukai DU2* M.M
1Department of Child Health Care, Hubei Maternal and Child Health Hospital, China.
2Department of Maternal Health Care, School of Public Health, Tongji Medical College, Hua Zhong University of Science and Technology, China.
3Department of Maternal & Children Health Care and Adolescent Hygiene, Family Planning Service Center in Jinan, China.
4Department of technical guidance, Family Planning Service Center in Jinan, China.
*Correspondence:
Yanqin WANG M.B., Department of Child Health Care, Hubei Maternal and Child Health Hospital, Wuhan, China, E-mail: yqwang1224@163.com.
Yukai DU, Department of Maternal and Children Health Care and Adolescent Hygiene, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei province, China, E-mail: duyukai2000@163.com.
Qiong Dai and Jianqiong Liu contributed equally to this work.
Received: 29 September 2018 Accepted: 01 November 2018
Citation: Qiong DAI, Jianqiong Liu, Bei LIU, et al. Study on the Relationship between Coping Style, Social Support and Quality of Life in Breast Cancer Surgery. Gynecol Reprod Health. 2018; 2(6): 1-5.
Abstract
Objective: To assess the relationship between traits coping style, social support and Quality of Life (QOL) of breast cancer surgery by Canonical Correlation Analysis (CCA).
Methods: 400 breast cancer surgery before a week were interviewed with traits coping style questionnaire (TCSQ), social support rating scale (SSRS) and Chinese Version of functional assessment of cancer therapy (FACT-B V 4.0), in which they were asked to recall major events and their corresponding feelings.
Results: There was statistical significance for the model of CCA (P<.0001). The first set of linear combination of typical variables after standardization, the standardized linear combination of the first pair of typical variables are as following: V1=0.5466 x1-0.1499 x2+0.5107 x3+1.1313 x4+0.3916 x5+1.3175 x6. The second set of linear combination of typical variables after standardization, the standardized linear combination of the first pair of typical variables are as following: U1=-0.3402y1+0.2092y2+0.1619y3+0.0322y4-0.1358y5+0.9530y6.
Conclusion: Traits coping style and social support were associated with QOL of breast cancer surgery.
Keywords
Introduction
Breast cancer treatment causes permanent physical problems due to the type of operation used. Although many women choose to undergo mastectomy and express no interest in breast conservation or reconstruction, for most women loss of a breast is an emotionally disturbing and difficult circumstance. With modern medical model transforming from biomedical model to biology- psychology-community medical model, the therapy no longer simply emphasizes the elimination of tumor and prolongation of life span, at the same time, the improvement of the quality of life is emphasized as well [1]. Because long-term survival is common among women with locally advanced breast cancer, quality-of- life issues become vitally important.Quality of Life (QOL) has long been an explicit or implicit goal, adequate definition and measurement have been elusive. Diverse objective and subjective indicators across a range of disciplines and scales, and recent work on subjective well-being (SWB) surveys the psychology of happiness have spurred renewed interest [2]. Owing to the fact that success of treatment in prolonging life is a mixed blessing-it is not enough to survive, patients also want to live [3]. QOL is presently an important factor in oncology research [4]. QOL and its components and determinants have received growing interest [5-9] and physical, mental and social well-being, with varying levels of emphasis in various combinations, have been included in the concept [3,5,10,11]. As a whole, women who remain free of breast cancer seem to have levels of functioning and quality of life that are in comparable to those of the general female population, although those who receive systemic adjuvant chemotherapy may do less well [12]. As a result, study for patients' QOL was increasingly emphasized. Over the past decades, there has been increasing interest in the association between psychosocial factors and breast cancer risk. Enhancing QOL has long been a major explicit or implicit life-style and goal for patients with breast cancer. Several studies have examined QOL of patients with breast cancer. Although there appears to be consistent evidence which link psychosocial characteristics and QOL of patients, the impact that coping style and social support on QOL was inconsistent.
Psychosocial factors have been increasingly regarded to impact to the QOL of cancer patients. Different coping style and social support may be present when women are diagnosed with breast cancer. The psychological definition of coping is the process of managing taxing circumstances, expending effort to solve personal and interpersonal problems, and seeking to master, minimize, reduce or tolerate stress or conflict [13]. Social support is the physical and emotional comfort given to us by our family, friends, co-workers and others, and is often used in a broad sense, including social integration[14]. Social integration refers to the structure and quantity of social relationships, such as the size and density of networks and the frequency of interaction, but also sometimes to the subjective perception of embeddedness. Social support refers to the function and quality of social relationships, such as perceived availability of help or support actually received. Social support in the narrow sense has been defined in various ways. For example, it may be regarded as resources provided by others, as coping assistance or as an exchange of resources. On the basis of these facts, the study was to assess the relationship between trait coping style, social support and QOL of breast cancer surgery.
Materials and Methods
Study population
Women aged 23-80 years, diagnosed with the first, pathologically confirmed breast cancer between June 2013 and May 2015, were identified in three hospitals, including Tongji Hospital, Xiehe Hospital and the Wuhan Central Hospital in Wuhan City, Hubei Province of China. Among the 400 women included in this analysis, 25.30% had at least a college degree; 55.75% was employed, 16% was unemployed and 26% was retired; 88.70% are the first marriage, 66.50% are from urban areas of Wuhan City and 33.5 % are from the rural areas of Wuhan City.
Data collection
Face-to-face interviews were conducted in the in-patients of the three hospitals--- Tongji Hospital, Xiehe Hospital and the Wuhan Central Hospital. Interviewers were trained in survey and mental assessment methods. Information on demographic characteristics (ethnicity, residence) and marital status was ascertained directly from the subjects. All participants who were operated before a week were interviewed with traits coping style questionnaire (TCSQ), social support rating scale (SSRS) and Chinese Version of functional assessment of cancer therapy (FACT-B V 4.0), in which they were asked to recall major events and their corresponding feelings.
Psychosocial Measures
Three questionnaires were administered as following:
Social support was measured by the social support rating scale (SSRS). The SSRS, a 10 items, is to assess the four levels of score, objective and subjective support, utility degree of social support, and measures perceived availability (the number of people that the individual thinks he or she can count on, if necessary) and satisfaction with perceived social support.
Coping style was measured with traits coping style questionnaire (TCSQ) designed by Dr. JIANG Qian-jin and the results were presented as positive coping score (PC) and negative coping score (NC). The TCSQ composed of positive coping and negative coping, and each factor was respectively composed of 10 items, the scores on coping styles were assessed by the difference between negative coping and positive coping. The higher the scores, the more negative the coping styles were. The extent to which each item has been experienced is rated on a 5-point scale, ranging from 1 (very positive) to 5 (very negative).
Quality of life (QOL) was measured with Chinese Version of functional assessment of cancer therapy (FACT-B V 4.0) scale that was composed of additional concern and FACT-G scale, which was developed and validated by Cella et al. and was translated into traditional Chinese due do culture-dependent of QOL and tested by WAN Chong-hua, et al in 1998. FACT-B V 4.0 is a self- administered instrument designed to assess multi- dimensional aspects of the QOL in breast cancer patients. It consists of 27- item FACT-General (FACT-G) and 9-item additional concern. The FACT-G assesses four primary dimensions of QOL, including physical well-being (7 items), social and /family well-being (7 items), emotional well-being (6 items), and functional well-being (7 items). A five point Likert-type response scale ranging from 0 to 4 is used (0 = 'not at all'; 1 = 'a little bit'; 2 = 'somewhat'; 3 = 'quite a bit'; and 4 = 'very much').
All data was carried out by SAS 9.0 software. Descriptive statistics were calculated for all variables. Descriptive statistics were calculated to describe the characteristics of the participants and the scores of each item of the SSRS, TCSQ and FACT-B V 4.0 scale. All data was presented as mean±standard deviation (SD). Canonical Correlation Analysis (CCA) was used to assess the relationships of life events, social support, coping style and Quality of life. P value less than 0.05 was considered statistically significant.
Results and Discussion
Results
Associations between each of the 12 independent variables in independent 3 questionnaire—traits coping style questionnaire (TCSQ scores), social support rating scale (SSRS scores) and Chinese Version of functional assessment of cancer therapy (FACT-B V 4.0) scale —were examined separately at the different points of assessment as shown in Table 1.
NOTE: F Statistic for Roy's Greatest Root is an upper bound.
There was statistical significance for the model of Canonical Correlation Analysis (CCA)( P<.0001).
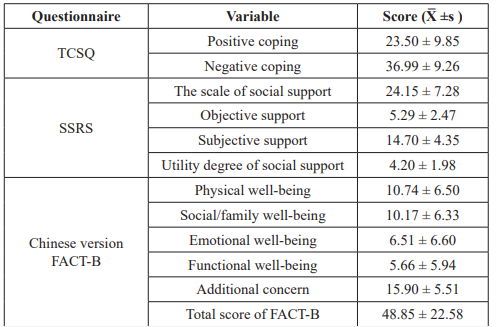
Table 1: The scale of TCSQ, SSRS and FACTB (XÌ? ± s)
Table 2 shows the relationship of TCSQ SSRS and FACTB with breast cancer by canonical correlation analysis. Psychosocial factors in TCSQ(x1: positive coping and x2: negative coping) and SSRS(x3: the scale of social support, x4: subjective support, x5: objective support and x6: utility degree of social support) are as independent variables, and items in FACT-B (y1: physical well- being, y2: social/family well-being, y3: emotional well-being, y4: functional well-being, y5: additional concern and y6: total score of FACT-B) are as the dependent variables.
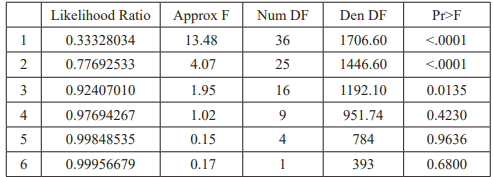
Table 2: F Approximations of coefficient in the canonical correlations.
There was statistical significance in the first three pairs of canonical correlation coefficients trend (F-test, P<.0001, P= 0.0135 respectively). There was no statistical significance for the later three pairs of canonical correlation coefficients trend (F-test, P=0.4230; P= 0.9636 and P= 0.6800 respectively). Although the first three pairs of canonical correlation coefficient were statistically significant, the first canonical correlation variables is the highest possible correlation between any linear combination of the variables in the predictor set and any linear combination of the variables in the outcome set. Therefore, the first canonical correlation of variables is chosen for study.
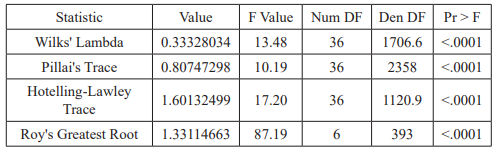
Table 3: Multivariate Statistics and F Approximations.
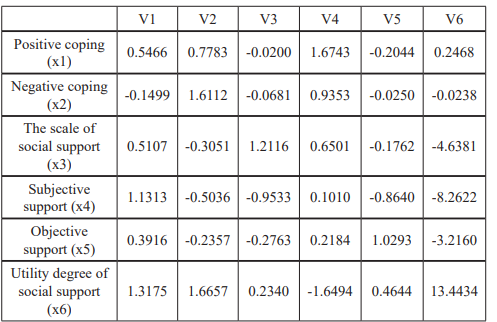
Table 4: Standardized Canonical Coefficients for the VAR Variables.
The first set of linear combination of typical variables after standardization, the standardized linear combination of the first pair of typical varibles are as following:
V1=0.5466 x1-0.1499 x2+0.5107 x3+1.1313 x4+0.3916 x5+1.3175 x6.
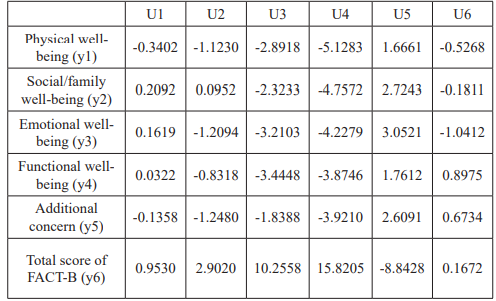
Table 5: Standardized Canonical Coefficients for the with Variables.
The second set of linear combination of typical variables after standardization, and the standardized linear combination of the first pair of typical varibles are as following:
U1=-0.3402 y1+0.2092 y2+0.1619 y3+0.0322 y4-0.1358 y5+0.9530 y6.
Discussion
Canonical Correlation Analysis (CCA) is a well-known technique for finding the correlations between two sets of multi-dimensional variables. It projects both sets of variables into a lower-dimensional space in which they are maximally correlated. The aim of this study was to assess trait coping style, social support as prognostic indexes applied to a defined Quality of life (QOL) of breast cancer patients after operation.
The surgical treatment of breast cancer lends itself to quality-of- life evaluations because both the disease and its treatment can be devastating. The study has shown that Quality of life (QOL) may be significantly affected following the diagnosis and treatment of breast cancer [15,16]. The result of this study showed that trait coping style and social support were associated with QOL (P<.0001). We suggest that not only treatment but also trait coping style and social support are associated with QOL. The fundamental principle behind CCA is the creation of a number of canonical solutions, our study showed that a linear combination of one set of variables, which has the form: V1=0.5466 x1-0.1499 x2+0.5107 x3+1.1313 x4+0.3916 x5+1.3175 x6 and a linear combination of the other set of variables, which has the form: U1=-0.3402 y1+0.2092 y2+0.1619 y3+0.0322 y4-0.1358 y5+0.9530 y6.
The results of this study showed that the correlation between coping style, social support and QOL were indicated the relationship between subjective support, the utilization of the support group in the first group and the total score of QOL in the second group Except negative coping, other variables in the first group were correlated positively with variables in the second group except the physical well-being and additional concern.
We found one who has positive coping style and higher utility degree of social support would be more positive, such as coping with illness and be optimistic, and are not nervous and don’t worry about worsening condition as to accept treatment positively. Similarly, Bonnie L. Green [17] reported that the findings highlight the important roles of trauma history and recent life events in adjustment to cancer and have implications for screening and treatment. Candyce H [18], reported that socially isolated women had an elevated risk of mortality after a diagnosis of breast cancer due to a lack of access to care, specifically beneficial caregiving from friends, relatives, and adult children.
The result of this study showed that social/family and emotional well-being have great impact on QOL. So psychological issues and family functioning continue to be a source of great effect for women with breast cancer. Compared with other samples of patients, women with recurrent breast cancer had poorer physical, functional, and emotional health whereas they had more pain, worry, role limitations, and symptomatic distress and a more negative appraisal of their illness as well. Clearly, these women are badly in need of care programs that will help them to manage these severe effects of the recurrent cancer so as to improve their quality of life. At present, there is a trend towards early discharge of hospitalized cancer patients to their private homes, thus leaving more of the care to the persons closest to the patient [19]. This trend is in line with the fact that patients hope get more concerns from their families. At home the primary caregiver (PC) is the main provider of physical and emotional support for the patient. PCs are mostly the patient’s spouse, partner or closest relatives, but significant others can also take on that role and function. We presume that one who gets support from her family and friends can cope better with side effects, such as premature onset of menopause, weight gain, and loss of libido, and so on. What’s more, Laurel L [20] reported that women with recurrent breast cancer are in need of programs to help them to overcome the severe effects of the disease to improve their quality of life. Programs needed include family members to help counteract the negative effects of the recurrent disease on their mental health, and to enable them to continue as effective caregivers. Thus, family and friends should be concerned with patients so as to help them get better QOL and prolong survival. As P. N. Butow [21] reported that quality of life is itself related to longer survival.
The result of this study showed that physical well-being and additional concern were correlated negatively with QOL. The higher score of physical well-being and additional concern showed that patients feel worse physical well-being, such as lack of energy, nausea, pain, side effects, illness perception, having to spend time in bed, and so on…At the same time, the result of this study also showed that negative coping was correlated negatively with QOL. In fact, the surgery of early-stage breast cancer has the potential to be stressful and to evoke a wide range of psychological reactions. Patients deal with a number of negative experiences, including medical treatments and their side effects such as fatigue, pain, and hair loss; temporary and permanent changes in physical appearance; alterations in future life plans; and the threat of future disease recurrence. These experiences may evoke negative psychological reactions. Due to the lack of capacity to negative emotional catharsis, the tensions linked to the strongest emotion convey and derail in the body. Suppression of negative emotions induced by a stressor might be associated with immunological changes, which, in turn, speed up the evolution of the disease [22]. Although more research is needed to establish whether these effects reduce recurrence or increase survival [23,24]. What’s more, G. Manna [25], reported that the subjects affected with mammary carcinoma have a reduced capacity to control their emotions and tend to use rigid reaction mechanisms to stress (negation or repression) and to interject aggression. Weihs [26] also found that restriction of emotion predicted higher mortality in recurrent breast cancer. In short, the adaptation to particularly stressful situations is the flexibility in the use of coping strategies to release negative emotion. Thus, evoking patients’ positive psychological can cover the gamut from existential changes such as vastly altered views about spirituality to behavioral changes and help to increase their QOL.
What’s more, we have tried to reduce sampling bias by recruiting from three hospitals serving a defined catchment area, and by making an initial contact with participants in the breast surgical ward so that losses and refusals were reduced to a minimum. To reduce reporting and measurement bias, we used two interviewers and ensured that borderline events and difficulties were rated at consensus meetings, and that equivocal stressors were rated by a third person unaware of the diagnosis. Apart from this, we avoided subgroup reanalysis, restricting our study to the association between onset of breast cancer and the experience of four types of stressor, which were specified before data were collected.
However, like all case-control studies, it has potential limitations. For example, the results could have been affected by recollection bias because the women were asked to recall past events and social support at that time.
Despite these limitations, our study shows that trait coping style and social support were associated with quality of life (QOL) of breast cancer surgery. To prolong survival, it is essential to decrease negative life events, reduce the negative emotional response and increase social support. Because the individual’s perception of the impact of breast cancer may change over time and the number of long-term survivors of breast cancer will further increase, further studies addressing the long-term consequences of breast cancer are warranted.
Acknowledgments
Special thanks go to all the patients who participated in the study. This work was supported by grants from Tongji Hospital, Xiehe Hospital and the Wuhan Central Hospital.
References
- Gai XL, Fan ZM, Jacques B. Comparison of survival among patients with breast cancer treated at first teaching hospital, Changchun, China, and Saint-Sacrement Hospital, Quebec, Canada. Chinese J Cancer Res. 1995; 7: 197-205.
- Costanza R. Quality of Life: An Approach Integrating Opportunities, Human Needs, and Subjective Well-Being. Ecol Econ. 2007; 61: 267-276.
- McDowell I, Newell C. Measuring Health. A Guide to Rating Scales and Questionnaire. 2nd ed. New York: Oxford University Press. 1996.
- Lehto US, Ojanen M, Kellokumpu-Lehtinen Predictors of quality of life in newly diagnosed melanoma and breast cancer patients. Annals of Oncology. 2005; 16: 805-816.
- Batel-Copel LM, Kornblith AB, Batel PC. Do oncologists have an increasing interest in the quality of life of their patients? A literature review of the last 15 Eur J Cancer. 1997; 33: 29-32.
- Velikova G, Stark D, Selby P. Quality of life instruments in oncology. Eur J Cancer. 1999; 35: 1571-1580.
- Osoba D. What has been learned from measuring health- related quality of life in clinical Eur J Cancer. 1999; 35: 1565-1570.
- Fatigue in cancer. BMJ. 2001; 322: 1560.
- Trask PC, Paterson AG, Hayasaka S. Psychosocial characteristics of individuals with non-stage IV melanoma. J Clin Oncol. 2001; 19: 2844-2850.
- Moinpour CM, Feigl P, Metch B. Quality of life end points in cancer clinical trials: Review and J Natl Cancer Inst. 1989; 81: 485-495.
- Osoba D. Lessons learned from measuring health-related quality of life in oncology. J Clin Oncol. 1994; 12: 608-616.
- Caroline B, Victoria C, Sharon Depression and anxiety in women with early breast cancer: five year observational cohort study. BMJ. 2005; 330: 698-702.
- Sharon GL, Yael Caspi Personality Traits, Coping Style, and Perceived Threat as Predictors of Posttraumatic Stress Disorder after Exposure to a Terrorist Attack: A Prospective Study. Psycho Me. 2006; 68: 904-909.
- Friedman LC, Kalidas M, Elledge R. Optimism, social support and psychosocial functioning among women with breast cancer. Psychooncology. 2006; 15: 595-603
- Irene LW, Ronald PC, Ralph SG. Differences in Quality of Life after Breast Cancer Ann of Sur Oncol. 1999; 6: 359-366.
- Kelly MM, Kelly KH. Neoadjuvant Chemotherapy, Locally Advanced Breast Cancer and Quality of J of Clin Oncol. 1999; 2: 441-444.
- Bonnie LG, Janice LK, Julia HR, et al. Epstein, Patricia Stockton, Ilyse Spertus, and Nicole Stern. Trauma History as a Predictor of Psychologic Symptoms in Women with Breast Cancer. J of Clin Oncol. 2000; 5: 1084-1093.
- Candyce HK, Laura DK, Eva SS, et al. Social Networks, Social Support, and Survival after Breast Cancer J of Clin Oncol. 2006; 24: 1105-1111.
- Grov EK, Dahl AA, Moum T, et al. Anxiety, depression, and quality of life in caregivers of patients with cancer in late palliative phase. Ann of Oncol. 2005; 16: 1185-1191.
- Laurel LN, Darlene M, Trace K, et al. Quality of Life of Women with Recurrent Breast Cancer and Their Family Members. J of Clin Oncol. 2002; 19: 4050-4064.
- Butow PN, Coates AS, Dunn SM. Psychosocial predictors of survival: Metastatic breast Annals of Oncology. 2000; 11: 46-74.
- Cousson-gelie F, Bruchon-schweitzar M, Dilhuydy JM. Do Anxiety, Body Image, Social Support and Coping Strategies Predict Survival in Breast Cancer? A Ten-Year Follow-Up Study. Psychosomatics. 2007; 48: 3.
- Luecken LJ, Compas Stress, coping, and immune function in breast cancer. Ann Behav Med. 2002; 24: 336-344.
- Lindad C, Roger JB, Melanie S, et Cognitive and Affective Determinants of Decisions to Attend a Group Psychosocial Support Program for Women with Breast Cancer. Psycho Med. 2005; 67: 584-589.
- Manna G, Foddai E, Di MM, et Emotional expression and coping style in female breast cancer. Ann of Oncol. 2007; 18: vi77-vi80.
- Weihs KL, Enright TM, Simmens SJ. Negative affectivity, restriction of emotions, and site of metastases predict mortality in recurrent breast J Psychosom Res. 2000; 49: 59-68.